In Pakistan, transparency has not been a hallmark of the Ministry of health in response to COVID19. Public criticism has mounted about the government apathy in recognizing threats of the pandemic, a complete lack of strategy, and an unclear source of research on the ongoing crisis. People who lost their loved ones due to COVID19 do not know the difference between civil and military; they only know the pain. This led to undermining the public’s trust in health experts and science itself.
The Pakistani government is hardly alone in its strategy for deflecting attention from its poor performance, from the US to India, from Trump to Moodi, many rulers have been acting incompetent, disseminating falsehood and fear exploitation for distracting public’s attention from government deficiencies in response to the pandemic. PM Khan’s playbook is downplaying the severity of the threat since March 2020, and he has been disregarding scientific evidence that supports the critical role of social isolation and lockdown measure.
The healthcare system of Pakistan is in a complicated phase due to decentralization. However, to address the devolution of power between the federal government and provinces, the parliament of Pakistan had passed the 18th amendment bill on 20 April 2010. Taking this into account, the provincial Assemblies took active steps and passed their own healthcare bills to ensure promulgation of equity and quality to the healthcare services and improvement in access to safe medical services. After individually passing such highly aimed bills, the health indicators still lag behind in achieving set targets.
In the health financing domain, the federal government is expanding 25 billion PKR that has been doubled from the previous year’s health budget of 12 billion; still, it carries only 0.4% of GDP. The health force indicates insufficient staff; there are approx—1:1300 doctor-patient ratios, which is lower as recommended by WHO. According to the available statistics for the delivery of medical services, there is an entire absence of programs and initiatives for non-communicable diseases at provincial and federal levels. Almost 78% of the general population pays out of their pockets for medical treatment.
Meanwhile, the statistics marked more than 2, 50,000 COVID19 positive cases with around 4500 death toll, the pandemics threw detrimental effects on healthcare. The ongoing situation has highlighted some criticalflaws in our healthcare system that includes but not limited to a scarcity of proper diagnostic facilities in hospitals, an insufficient workforce, and mismanagement of medical education and practices, especially in remote areas.
There lies a strong bonding between the human workforce and the patient’s safety. As we all recently witnessed, the paramedical staff and doctors are fighting this infectious disease on the front line, stepping out of their comfort zones, enduring painful experiences, and risking their lives to do everything to save our lives.
Pakistan has a pretty diverse healthcare system from tertiary care centers down the roads to primary healthcare centers, but unfortunately, they have lost their credibility at the hands of ill-administration. From posh areas of Karachi and Lahore to far-flung districts of Baluchistan, resource constraints are one of the primary barriers to quality medical services. The mal-governance, negligence, unjust, and unaccountability are the deadly poisons that restrict more allocation of local resources and wound existing ones.
According to a recent survey, in Pakistan, there exists a slight imbalance between private and public healthcare setups in terms of the burden of patients. The primary and secondary healthcare centers, especially in pre-urban and rural/remote areas, have been quite famous for the absenteeism of medical staff and doctors with an entire lack of basic medicines and diagnostic equipment. Therefore, the mal-functioning of primary and secondary healthcare centers has ripple effects and people are forced to take their patients to the tertiary centers, which are mostly located in big cities like Karachi, Lahore, Rawalpindi, and Islamabad.
Although Pakistan has given birth to some notable, globally recognized doctors, surgeons, researchers, and physicians, without question, there were and are severe deficiencies in our healthcare systems. The WHO ranked 195 nations on the overall quality of healthcare services, and interestingly Pakistan ranked 154th, stays behind its South Asian counterparts India (145), China (47), Bangladesh (133), and Sri Lanka (71).
It is evident that the system is leaking at seams, yet politicians are immobilized by ideology, fear of being voted out of the office. The government’s poor policies in healthcare resulted in the scarcity of choices regarding effective diagnostic and medical services. Something has to change, and it has to change quickly; otherwise, if another epidemic or virus outbreak hits the country shortly, the overloaded healthcare system will cripple. The Government should have to work for us—our lives depend on it.
Often heralded as the messiahs for those most in need, doctors in Pakistan have held a reverence few could claim. The profession itself has been glorified for decades. While one can argue as to the validity of this status and doctors themselves might feel patronized as a result of it- one thing is for sure, this status of glory is slowly waning away.
Recent times have sparked repeated cases of healthcare professional assault and public hospital property being thrashed by violent attendants. Patients will always blame the physicians and physicians will continue to change the way they practice in return, afraid for their safety. While such incidents can only be condemned in the strongest of languages, it seems as though we’re all unanimous on one thing. Such incidents are a sign of a failing system.
Public healthcare in Pakistan has long been neglected. One only has to visit a tertiary care public hospital to realize the multitude of problems we need to address. Let us, however, divide these problems and the threats they pose in two major categories- issues internal to the infrastructure of the hospitals and those external to it. The debacle isn’t as nuanced as this; however, we shall try to make it as simplistic as possible.
The federal government estimates a considerable percent of the total fiscal year budget to healthcare. Provincial governments further allocate the budget to various healthcare departments. As a struggling economy with a GDP growth rate of 2.6%, the budget allocated to healthcare is inadequate. But how do we truly know that the budget is inadequate and it is not, as one would assume in a country fighting corruption, a case of money being channeled to fill pockets of those in charge? While it is true that each year billions of rupees are allotted to schemes and projects that only exist on paper, the fact is that it’s not our only problem.
Pakistan has an ever-growing population. It is the 5th most populated country and for the state of its economy, this does not bode well. Lack of resources is doubled when the demand for those resources increases. As an intern in one of Pakistan’s busiest tertiary care hospitals, it was not uncommon to see medications run out of stock each day. One would have to write requests to NGOs working on donations and they would waive a portion of the cost. Patients would then be expected to buy these medications. For starters, transparent, accountable investment is key to developing a good healthcare system.
In January 2018, I had the chance to visit Tharparkar and adjoining towns for awareness sessions in collaboration with a relief eye camp. While on our trip, we were shown around the town and then taken to the local Civil Hospital of that town. The plan was to use one of the wards there for our sessions. The sight that awaited us was one I can never forget. The hospital was a ghost town. There were no patients, doctors, infrastructure except a yellow-walled building crumbling before us.
There was a massive pool of sewerage water right beside the entrance, there was a shiny new board in the basement claiming to be a Protection House for Women but by the looks of it was exactly the kind of place any woman would seek protection from. There was one room that had multiple hospital beds. I looked inside and there was a nest of pigeons in one of the mattresses. The gory details of this hospital are many. As an intern in Karachi’s Civil Hospital, I could yet again see from miles away how these hospitals in small towns functioned because patients from far off would come to us braving days of travel with things as urgent and basic as snake bites and dog bites. The structure of healthcare goes like this – you have primary healthcare i.e. your local general physician.
The doctor to patient ratio in Pakistan in appalling. (Image Credits: www.qoura.com)
Then you have secondary healthcare which is a multidisciplinary community setup. And lastly, we have tertiary care hospitals like Civil, Jinnah, Agha Khan Hospital, to name a few. The setup ensures that tertiary care hospitals aren’t overburdened with cases that can be easily handled by a primary care physician. It ensures that a patient can receive initial care and be stabilized before they’re referred to a tertiary care hospital if need be. Lack of proper primary care and secondary care setups places all the burden on our tertiary care hospitals.
There must be regulated, monitored and PMDC certified primary care setups as well as secondary care setups. This is even more important in the case of trauma. Trauma is the leading cause of mortality worldwide and in Pakistan, it is even bigger of a burden as it causes death and disability in the country’s GDP-dependent population. According to Dr. Haris Sheikh, who worked extensively for First Response and Mass Disaster in Karachi, “ a central EMS system with equipped ambulances and trained paramedics, a functional disaster management cell and a Level 1 trauma center is essential when it comes to trauma care. The clock starts ticking the moment trauma occurs.
Keeping in mind the concept of golden hour, necessary steps can be taken even before a casualty reaches the hospital, the most important of which are resuscitation and activating essential services like CT, Cath lab, or even ORs with appropriate teams ready to take care of the casualty upon arrival. Sadly, none of the aforementioned essential services exist in our system resulting in on-site manhandling of casualties and a delay in the in-hospital treatment, which in certain circumstances can prove catastrophic”. This brings us to the second half of our problem- in hospital inadequacies.
Impediments to healthcare within hospitals are multifold and apparent to anyone who has set foot in public hospitals. The plot gets thicker for those who have worked in the healthcare system. Apart from the significant roadblock coming from lack of resources and inadequate systems, the infrastructure of most tertiary care and secondary care hospitals lacks cohesion. For instance, a patient presenting to the ER must undergo triage, be assessed further, admitted if need be, or set up for an appointment at a later date.
There is an evident lack of assignment of duties and protocols and a lot is left up to the decision-making of the doctors on calls. Diagnostic services are often absent and patients have to run back and forth for getting tested. For example, it is not uncommon to find the CT scan machines and MRI machines at Civil Hospital Karachi in non-working condition for months. Patients, even those who have sustained traumatic injuries and need urgent head CTs or have had a stroke and need immediate assessment for life-saving treatment, have to be referred to other places to get a CT scan. Similarly, most tertiary care hospitals do not have 24/7 Cath Lab services for patients reporting with MI or heart attack as it is commonly known and has to be referred to centers like NICVD and Tabba. A lot of this also has to do with a lack of trained personnel, which in itself is a multi-faceted problem.
The doctor to patient ratio in Pakistan in appalling. We need newer training positions for physicians, regular board exams to ensure they are up-to-date, accountability systems, and recruitment of paramedical staff, which is not only limited to nursing but can create space for respiratory therapists, perfusionists, physiotherapists, pharmacists, etc. This allows a more holistic approach to treating the patient. Perhaps most importantly, job satisfaction amongst healthcare providers, be it nurses or doctors is shallow in public hospitals. Their salaries and stipends aren’t regular; their employment offers no perks nor insurance of any kind, working hours are indefinitely laborious, facilities provided at work are subpar and would shock most people at the inhabitable state of on-call rooms and most days, they are also afraid for their safety and security while at work.
Those in power continue to turn a blind eye to these problems and very little importance is given to attempt to change things. In fact, change is almost scorned at. While the rest of the world looks at Artificial Intelligence and 3D printing to facilitate medical diagnostics and therapeutics, hospitals in Pakistan barely have a well-integrated IT system to record patient information and regulate drug prescriptions. The fact that some of the well-run departments in our public hospitals are those being run on charity, donations, and efforts of philanthropic people is a silent but persuasive reminder of the inefficiency of the administration. SIUT, NICVD, PWA are all such brilliant examples.
Healthcare, like education, is currently struggling in Pakistan. While there is so much to be done, we have hope. New doctors are joining the force each day and new organizations are always on the front running blood banks, pediatric emergencies, and sourcing funds for patients. Ever abysmal situation has heroes and so does ours. We just need to know where to start and have the will power to do so.
Malaria is one of the most devastating parasitic diseases in Pakistan. In the past few decades, malaria transmission was highest in Pakistan’s northern part, especially in Khyber Pakhtunkhwa province. Bannu district, located in the southwest of the KPK, is a malaria-endemic area in Pakistan. Bannu is densely populated, and the high influx of Afghan refugees has exacerbated the malaria problem here.
A couple of malariometric cross‐sectional surveys were conducted in Bannu to evaluate malaria infection during the past two decades. According to that, PCR is more accurate than microscopy when it comes to specie analysis of a pathogen. In Bannu, genetic analysis of malarial parasite Plasmodium was performed. P. vivaxwas a dominating pathogen in 83.3% of cases. While 24.6% of malaria cases were caused by P. falciparum, the co-existence of both species was seen in 28% of clinical malarial samples. In comparative microscopy, poor diagnosis and differentiation of species on microscopy P. vivax were 68.4% versus 31.6% P falciparum, while total misdiagnosed cases were ~15% of the cases.
Some other epidemiological studies have been conducted in other areas of Pakistan. Still, the investigation of malaria transmission on a nationwide scale has been hindered by the shortage of data from several areas. Though, it is evident that the primary reason for the high mortality of Malaria between August and October 2015, which is the peak season for malaria transmission, is the poor diagnosis, inadequate sanitation, and lack of high-quality healthcare and blood testing facilities in various parts of Pakistan specifically in KPK, Baluchistan, rural Sind and Punjab.
A report published in Daily Dawn on 5 June 2020 that two persons, Attiq u Rehman of Kot Usman Khan and Tanvir of Sohandin locality in Punjab, buried with Coronavirus SOP later tested negative. Such incidents sparked some heated debates on social media. They brought about some harsh realities that how ill-mannered our society has become and equally highlighted some significant defects in diagnostic tools and laboratory testing in Pakistan.
Healthcare spending in Pakistan has been on the rise since 2002. According to the data released by the Pakistan Bureau of Statistics, consumer spending on health care was estimated at 378 billion PKR, which does not include the government’s spending on healthcare. After the pandemic hit the country hard, the current government increases the budget for healthcare to 6.4 billion in the newly announced budget of 2020.
The healthcare spending in Pakistan has been on the rise since 2002.
Meanwhile, the diagnostic appears to be attracting considerable interest in the last three decades, and big names such as Agha Khan, Shaukat Khanam, Chughtai Labs, Armed forces institute of pathology, Dow diagnostic reference and research laboratory (DDRRL), Shifa, and others all are set to benefit from this shift. But eventually, this trend resulted in the dark plays when a considerable number of small labs started business on healthcare matters. “Statistics showed that there are more than 4000 labs with less than 400 qualified pathologists or experienced lab technologists in Punjab alone. So one can imagine the things being done to the public in the name of pathology”, said Dr. Omar Chughtai, Director Operations of Chughtai labs.
“There could be several reasons behind the error in the reports of medical testing labs, like sampling, transportation error, and temperature difference maintained in the labs for preserving samples. Besides these technical errors, one can’t neglect the possibility of human error due to workload in hospital and testing labs these days”, said Syeda Fatima uz Zahra, a trainee for Total Lab Quality Management at a reputable lab in Karachi.
“Before March 2020, most of the well-reputed labs like DDRRL have had 300 0r 400 maximum cases and are now receiving 1200 to 1500 cases daily. Since the workforce is the same, it is obvious that the staff at hospitals and labs are experiencing overburden and overwhelming anxiety due to lack of PPE”, she added.
However, in many well-established laboratories like DDRRL and Agha Khan Laboratories, most of the work is automated. Once the sample is received and preserved, other processes of extraction, inspection, and preparation of reports all carried out by the machines. So, due to less interference of humans, there would possibly zero chances of error. Here, it is worth mentioning that many laboratories are using kits for testing Coronavirus that are not verified yet by the concerned authorities and are going through the trial phases. However, the PCR has 100% sensitivity and specificity. Typically, kits used for molecular diagnostics yield the best possible results. But due to overburden, somehow low-grade kits, research only kits, and primers are approved as toolkits. This method is recommended by the CDC and WHO for emergency use only. As there is no or less time for testing and demand for the kits is sky-high. These kits may have a bit higher error margin and false-negative results due to low sensitivity of up to 95%, but still, it is authentic, Zahra informed.
“Many labs are following the accreditation services; for example, Agha khan is a CAP (American Society of Pathology) recognized lab. So, whatever the test has taken by Shaukat Khanam is equivalent to any US lab that has the same certification. To maintain given criteria labs, have to keep them up to date. They exchange samples and a competent authority independently crosses check match results, ” said Mohammad Bilal Khan, a certified Lead Auditor, Quality Management System (Labs), and a Technical Advisor to SureBio Diagnostics and Pharmaceuticals.
An ISO that applies to the diagnostic Lab is ISO 15189. And quality labs seek these criteria. For this, there is a stringent standard to meet, and it includes proficiency testing. Indicates that an independent authority will verify your lab samples and reports, and you will be accredited only if your reports and results match the provided standards. The frequency of testing depends on workload and type of tests, such as the HBA1C test for sugar patients. For this test, equipment is calibrated daily. For CBC, mainly on the 7th day, the equipment is calibrated with control, but it is highly dependent on the workload. Of course, keeping up all standards comes at a cost, and small labs run by small ventures may not be able to afford it, so they do not prioritize it. Khan added.
In many well-established laboratories like DDRRL and Agha Khan Labortories, most of the work is automated.
The Laboratory testing is performed under federal and provisional government act too. Most labs seek calibration services from PNAC, PCSIR, and some other institutes that provide calibration services for equipment and testing. All equipment is calibrated. Mostly master calibration is performed by given institutes, for example, weighing equipment. A team of experts visits the lab and performs calibration there, and then, based on that, internal pieces of equipment are calibrated by the lab staff itself. The sophisticated equipment types are QC and inspected by the suppliers and service providers, like Thermo Fisher Scientific, which provides the safety cabinet responsible for its monitoring. Institutes sign contracts, and inspection is carried out annually. It is a requirement of the quality standard that all equipment must be running and logbook be well maintained, Khan told.
To dig deep about quality assurance standards in medical testing laboratories, we reached out to several lab technologists and experts around Pakistan. A lab technologist of Islamabad Diagnostic Center briefed that his lab provides state-of-the-art facilities, with imaging and lab services. The imaging modalities are connected through PACS, where medical experts from abroad are also involved in making Tele-diagnosis. Our nationwide branch network is currently providing the best quality diagnosis with a quick turnaround. We encountered similar statements from Dar ul Sehet Karachi’s lab personals, Al Shifa Karachi, Rahat Laboratories Quetta, Hayat Abad medical complex Peshawar. They claim for providing quality testing services with internationally applicable standards.
It might be possible that some of these labs running are struggling to maintain Quality assurance. Still, most of the small labs running in the residential areas around the country are taking these precautionary measures for granted. Some major problems are as below.
Use of substandard chemicals, reagents
Use of outdated equipment which is out of calibration
Use of sub-standardize Immuno-Chromatographic Testing devices
Ill trained and unprofessional staff
Mishandling of samples and violation of rules.
Absence of cross-checking by authorities.
The standard procedure for staff appointment is based on a critical review system in the competent labs. Here, I would like to mention Shaukat Khanam, where lab technologists are appointed after strict practical and oral examination, and their certification is frequently revised and upgraded. Their entry to the lab and handling of samples is subject to accreditation possession, which is granted after passing an exam taken every sixth month.
There are two types of quality control for lab equipment: Internal Quality Assurance (IQA) and External Quality Assurance (EQA). A lab staff or management itself is responsible for IQA check, whereas, for EQA, Pakistan has its own quality assurance institutions that are regularly monitoring their associated laboratory equipment and quality control. Like, the National External Quality Assurance Program of Pakistan (NEQAPP) is being run by AFIP, which endeavors to contribute quality in laboratories at the national level in the interest of public health and safety. The clinical labs have to register in NEQAPP; all the affiliated labs send their samples for testing that further analysis and a report been issued based on results and performances. But most of the labs running on small scales do not attempt to register in such institutions. Our health ministry neglected this nonsense situation for a long and never restricted small-scale labs to register or go for an inspection.
The complaints of negligence and malpractice in medical testing labs are not uncommon, however. The Law of Torts is invoked for a civil remedy for medical malpractice cases in Pakistan. Medical practitioners or lab technologists can be trialed under criminal liability charges, too, but our courts are very reluctant to treat them under Pakistan Penal Code and want to contest such cases under civil commitment. A separate law should be devised for medical malpractice, keeping in view the need and current practices of legal and healthcare systems.
Locusts are the primary agricultural pest of the world. Out of 5000 different species of grasshoppers, only nine species have been recognized as locusts. These nine species proved havoc for agriculture for years. We should have a clear understanding of the biological background, classification, impact on agriculture, marching time, and history of the invasion of locusts so that we can take steps about their control.
Before going into depths of Desert Locust, let’s have a look at its present attacks in Pakistan. National Disaster Management Authority said that Balochistan is the most affected area by the attack. A swarm of locust has spread to 52 districts of Pakistan, including 31 in Balochistan, ten districts in Khyber Pakhtunkhwa, 6 in Sindh, and five districts in Punjab. Fruit crops that have damaged by locust in Balochistan are apple, cherry, and peach, etc. It also ruined onion crops in Balochistan.
Desert Locust Schistocera Gregaria is known as one of the most voracious insects, which is polyphagous and can eat all types of vegetation that it comes across. Desert Locust is a species of swarming, migratory, short-horned locusts known to occur in desert areas with favorable agro-ecological conditions. Historically swarm of Desert Locust has always been a threat to agricultural production and food security in Africa, the Middle East, and Asia. This occasional pest produces two to three generations per year with a life cycle of 12 weeks. Almost 30 countries are potentially prone to Desert Locust, covering the area of about 16 million kilometers. In comparison, 60 nations are under the threat of invasion, covering the world area of about 29 million kilometers. This insect, after consuming the vegetation of an area migrates to another region where food is available to them.
Locusts show polyphenism i.e. they appear in two phases, gregarious phase and solitary phase.
Gregarious Phase: Crowding induces the gregarious phase and which is most notorious for its tendency to aggregate and form a massive swarm.
Solitary Phase: Isolation leads to the solitary phase in which individual activity avoids other locusts.
The differences between these two phases are collectively termed phase characteristics, extending from behavior and ecology, through morphology and anatomy, to physiology and biochemistry. Behavior can change within hours for some species, but other traits, such as morphology, can take several generations to shift entirely. This plasticity creates unique challenges; for instance, the gregarious phase locust, the Desert Locust, a single swarm can cover 1200 square kilometers.
One of the classifications of locusts is according to their feeding guilds,
Forbs and tree feeding locusts
Mix feeding locusts (grasses, forbs, and trees)
Grass-feeding locusts.
Desert Locust is a species of swarming, migratory, short-horned locusts known to occur in desert areas with favorable agro-ecological conditions. Photo courtesy of FAO/Sven Torfinn
Desert Locust is one of the mixed feeding locusts, and this tends to eat broadly from many plant families. This adaptation allows them to persist in and migrate through many landscape types. It also makes plagues a significant threat to livestock forages and pastures as well as the broad array of crops. This specie prefers overgrazed or disturbed habitats, potentially due to an increase in bare soil for lying egg and thermoregulation.
Gregarious locusts eat plants containing alkaloid hyoscyamine that solitarious locusts avoid and actively consume it, likely to gain gut-content mediated toxicity and avoid predation. Moreover, gregarious locusts are less discerning when faced with diet with nutrient imbalance as compare to solitarious locusts. It may be due to several reasons. Firstly, migrated individuals may encounter increased food diversity and this breadth may allow the gregarious individuals to redress nutrient imbalances. Secondly, groups of gregarious locusts may cross vast areas with no food, and a narrow host plant breadth may mean starvation. This diet expansion, in combination with aggregation likely heightens agricultural impacts. Indeed, locusts can cause 80 to 100% crop losses across affected areas.
A Desert Locust adult can consume roughly its weight i.e., about 2 grams of fresh food per day. The notorious 1915 locust attack in the Middle East, for example, resulted in wiping out a largely underestimated 536,000 tons of food. According to FAO, in modern days, African nations spent US 30 million dollars in anti locust campaign.
When an invasion occur all type of vegetations are subject to attack. Damage can be considerable on all types of crops: annual rain-fed crops as well as perennial crops, tree cultivations, and irrigated crops. Locally food competition between locusts and livestock leads to a deterioration of the vegetation and the soil. Locusts invasion can, therefore, lead to desertification at the local level. These invasions occur during periods when rainfall is highly favorable to the development of crops increases their economic impact.
Swarming is a hallmark of locust behavior. Swarming is a result of attraction and aggregation tendency of locusts in the gregarious phase. Locusts band will typically have one period of marching in the forenoon and another in the afternoon, strongly depend on weather conditions such as temperature, but also on clouds obscuring the sun, as well as on rain and cold wind. Mostly Desert Locust’s marching took place from just before noon to two hours before sunset. The marching band can cover very different areas, from a few hundred square meters to several kilometers. The shape of the marching band can also vary, ranging from columnar to frontal structure.
The Desert Locust crises started back to May 2018 when a cyclone passed over a vast unpopulated desert to the southern Arabian Peninsula, filling the space between the dunes with ephemeral lakes, which allowed locusts to breed undetected. This was further amplified in October 2018 by cyclone Luban, which spawned in the central Arabian Sea and then marched westward. Locusts grow exponentially in this kind of climate, and ultimately these two 2018 cyclones enabled three generations of wildly successful locusts breeding in just nine months, increasing the number of these insects roughly 8000 fold.
This article is written by Irfana Yasmin, who is a student of MSc Botany at Quaid-i-Azam University, Islamabad.
Astronomy is the oldest science we know. The sun, the moon, and the stars have been the fulcrum of our scientific stretch. We have been able to pinpoint ourselves in the universe with the help of a swarm of dedicated dweeby scientists who spend their life traveling in the corridors of science, seeking nothing but the truth. At present, advancements in technology have shrunk in a digital globe. Some people and organizations are working for the outreach of science to laypeople and enthusiasts. One such organization is Scientia Pakistan. Being a media body present on Web Space, Scientia sports a Digital Magazine Website show-casing the latest scientific breakthroughs and ventures. Here is Scientia, we aiming to spread scientific temper among people and keep organizing events to reward and promote scientific achievements.
In May 2020, amid the global lockdown due to the COVID-19 crisis, Scientia was approached by a leading astronomy club ‘RaheQamar’ for co-organizing an online astrophotography contest. Mr. M. Iftekhar Yezdani from Rahe Qamar is a well-known personality working for astronomy popularization in Pakistan. We underwent a glorious collaboration to host this contest, yielding some of the most stunning images ever captured by amateur astronomers around Pakistan. Entries were invited for over a month, and it’s was time to get them judged.
With some rounds of discussions, we (RaheQamar and Scientia) decided to bring on aboard the bests in the business. Dr. Salman Hameed, professor of integrated science and humanities, a Ph.D. in astronomy, graced the judges’ panel miles away from the US. Dr. Farrukh Shahzad, the founder of the Pakistan astronomers, one of the leading and oldest astronomy societies of Pakistan, was also among the judges’ panel. Our next expert to have graced as a judge was Mr. Umair Asim. The guy with his own Zed’s observatories in Lahore, Pakistan, and 30 years of astronomy experience. Upon leaving our participants under the observation of these connoisseurs, we enjoyed marveling at the brilliant images shot by our enthusiastic participants
As the month passed by, we kept on getting entries for the contest, and our esteemed judges engaged themselves in each of the images they examined. They admired the beauty and the uniqueness of the photos and the technical skills and the tools involved. And after severe discussions and intense examination, we had our set of winners, and it was time to unveil the curtains and announce the names.
On the evening of the 6th of July 2020, the announcement was embedded in a Webinar bringing up all the judges discussing STEM, STEAM, and Astrophotography. The webinar went LIVE on Facebook and astonishingly got overwhelming attention from people across Pakistan.
Winning photograph
Western Veil Nebula by Shoaib Usman Banday Cash Prize 6k
Runner Ups
Solar System Collage by Imran Rashid Cash Prize 3k
Partial Lunar Eclipse by Ali Abdullah Cash Prize 3k
Mr. Iftekhar Yezdani from RaheQamar moderated the event in an exciting ad way and was joined by Sandeep Poddar from India representing Scientia. Both the moderators sailed the boat with exceptional balance and fun. The panel discussed the wining images and their experiences while judging them. And the names of the winners were announced with great pomp.
The whole of the Scientia Team was having a great time behind the scene and was relived to watch their month-long hard work turning into such a big success. The online show got a warm reception by the astronomy community present over the online space.
Team Scientia feels blessed to have been a part of this venture and thanks RaheQamar for being our partners. We thank and convey our warmest regards to the experts who graced this event with their time and words. A big thanks to all the participants and winners, contributed with the best abilities, skills, and dedication to this venture. With support, we will keep breaking the barriers and reach beyond the boundaries of nations. After all, we all share the same sky!
On June 5 near Pusch Ridge in the Catalina Mountains north of Tucson, a lightning-sparked the bighorn fore that has resulted in evacuations and hundreds of wildfire fighters are fighting with. The fire erupts in Tucson close to overtaking the No. 7 spot Thursday for the largest wildfire in Arizona history and has claimed 118,710 acres in the Catalina Mountains and is 58% contained.
Mount Lemmon brightened after fire sparked, evacuations are under way
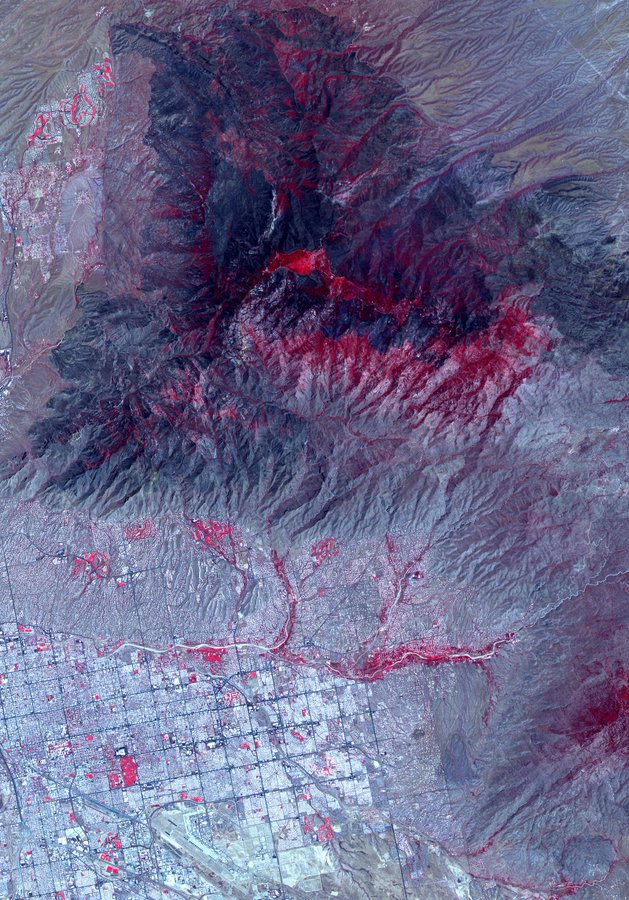
The Jet Propulsion Laboratory NASA has released some satellite images of Bighorn fire that show the Devastation from the #BighornFire burning north of Tucson, Arizona as seen from space by the ASTER instrument on the Terra @NASAEarth satellite. The blaze spans more than 114,000 acres and is at 45% containment: http://go.nasa.gov/3dL9DN2
Satellite image of the area covered bighorn fire
The fire burning on the Northside of Santa Catalina Mountains near Tucson this afternoon at about 4:30 pm. Mt Lemmon Fire station in the foreground is about 1/2 mile from the middle of the village of Summerhaven, which burned earlier in 2003.
A shot from my backyard near Grant and Swan. It’s got a lot of people’s attention in Tucson tonight.
The residents of Arizona are praying for the intermittent Rains
A new discovery of collision between a black hole and a mystery object has recently been made. The object in question is speculated to be a neutron star but its size is not big enough to be considered a black hole.
This discovery was made last year on August 14 by the gravitational wave detectors LIGO and Virgo. It was first thought to be a collision between a black hole and a neutron star but new research and study on the gravitational waves suggest that the case might be different. A report published on June 23 shows that the black hole was 23 times as massive as the sun and it hit a dense body of about 2.6 solar masses. This means that it is heavier than a neutron star but also smaller than the lightweight black hole. What it really is, is still in speculation.
Usually, when stellar explosions occur, neutron stars form as the residues. But there is a limit to their size. The cap is placed at 2.5 solar masses because stars bigger than this limit can breakdown under their own weight. And theoretically, black holes of sizes less than five solar masses are possible, but no such observation has been made yet.
There are not enough clues and traces for astronomers in this collision to identify the object and its more intimate features. The observation made by U.S.-based Advanced Laser Interferometer Gravitational-Wave Observatory, or LIGO, and its sister experiment in Italy, Advanced Virgo prompted other telescopes to hunt for more data, but they were not successful.
The lack of data may push towards the idea of considering this object to be a black hole because such collisions do not give off any light. At the same time, the neutron star hypothesis can also be an agreeable notion. The black hole may have devoured it in a way to be lost without a speck. According to Cole Miller, an astrophysicist at the University of Maryland in College Park, if the last sketch is true, “this means that [the pair of objects] had its moment of gravitational wave glory,” and bigger black hole forged in the collision is “doomed to wander the vast emptiness of space, probably never emitting another peep.”
In these troublesome days, one thing that we all have to understand and make a strong effort toward solving is knowledge accessibility. There’s no second opinion on the inefficacy of our education system, which has led to an immense social and economic disparity. It requires intervention on the scale of infrastructure, governance, and execution, but most importantly, it requires empathy.
The situation is quite unsure that even the World Health Organization has taken several U-Turns over its previous statements, and governments around the globe are struggling hard to save their people from the deadly Coronavirus. The Federal Government of Pakistan is having a hard time due to the severe lack of a plan and strategy for the pandemic. Baluchistan is one of these areas of the country, which is highly neglected in these days of trouble. But NGOs with their limited resources and collaboration of the Government of Baluchistan are working diligently for educating local people, especially of remote areas.
Balochistan Rural Support Program (BRSP) a non-profit organization working in Balochistan, is one of the largest organizations in the province. The organization was first evolved from the “Pak-German self-help project” in 1983, as a collaboration between the Federal Republic of Germany and the Government of Pakistan. Its main objective is to harness the potential of the rural low-income people by social mobilization strategy, helping them in their respective communities and to raise them up to their feet by improving their standards of living and also a sense of ownership for the local development. Currently, the organization has a presence in 26 districts of the province, focusing education, health, wash, capacity building & human resource, livelihood, and humanitarian relief.
The proud team of BRSP
On 10th March 2020, when coronavirus cases started ticking in Balochistan, Pakistan via Taftan border, and the first case confirmed in Quetta, the patient was a 12-year old boy, who had returned from neighboring country Iran with his family. As a result, on 20th March 2020, the government of Balochistan imposed complete lockdown in the province via issuing an official notification. Since then the organization carried its assessment and emergency response activities at 27 districts with the government of Balochistan by the support of international donors on the following six components.
Conducted awareness of COVID-19.
Strengthen capacity on COVID-19 infection prevention and control (IPC)
Adopted a resilient approach for its citizen, communities, government department staff, law enforcement personnel, and health care facilities through provision of PPE (personal protective equipment).
Increased WASH & Hygiene facilities specially hand washing units at public places.
Strengthened coordination with government officials and stakeholders for timely response on COVID-19.
According to Organization’s CEO Nadir Gull Barech, till now BRSP has reached about 6.76 million people of 940,263 households in 425 towns with rural councils of 27 districts (Barkhan, Chaghi, Dera Bugti, Duki, Harnai, Jaffarabad, Jhal Magsi, Kachhi, Kalat, Kharan, Khuzdar, Killa Abdullah, Killa Saifullah, Kohlu, Loralai, Mastung, Musa Khail, Naseerabad, Noshki, Pishin, Quetta, Sherani, Sibi, Sohbat Pur, Washuk, and Zhob) consisting an area of 243,576 km2 which becomes total 70% population of the province. He told dawn staff that when the COVID-19 disease first entered in Balochistan in March, the organization launched its mass awareness campaign for COVID-19 in district Quetta and other districts simultaneously through loudspeakers, masjid announcements, awareness signboards, orientation sessions, dissemination of IEC material & installation of handwashing facilities at public places. While showing the campaign individuals awareness data separately, he explained & recorded the following data;
Mobile loudspeakers announcements delivered messages in 3,983 hamlets of 425 UCs.
1,115 Masajid in 260 UCS recorded COVID-19 announcements via loudspeakers.
380,000 brochures/IEC distributed among citizens.
Awareness messages delivered by religious scholars through Eid Sermons at 23 locations in 7 targeted districts.
In addition, 1,893 CRPs (community resource persons) were Oriented and trained, who further reached out to 43,124 households in 199 UC of 15 districts.
On the other hands, 660 banners and 400 visibility boards including the large billboards installed on public locations and entrance of Quetta city.
Similarly,400 awareness-raising boards installed at the entrance of mosques in 7 districts.
Apart of this, COVID-19 awareness messages are being aired on FM 89 and local cable channels in Urdu and all local languages across the province.
Shortly, 1,000 copies of booklets written on “COVID-19 – Islamic Perspective on Pandemics” by BRSP distributed in 124 Madaris and Masajid in district Quetta.
Hygiene Kit distribution ceremony organized by BRSP
For strengthening capacity on COVID-19 infection prevention and control (IPC)
BRSP has trained and built capacity building of 61 health officials staff on COVID-19, said by the organization’s focal person on communication. He added that we have orientated 1,893 volunteers on COVID-19 Infection prevention and control (IPC) for their respective communities. Apart from this, 222 janitorial staff has been trained by BRSP on environment cleaning and disinfection principles for care facilities.
Adopting a resilient approach for its citizen and communities
BRSP has distributed 166,700 surgical masksamong its citizens., public & private health workers with the support of Indus Health Network. Similarly, the organization distributed 45,997 Sanitizers, 26,280 gloves, 40,964 soaps, and 2,911 protective suits. In addition, BRSP has also provided 1,320 hygiene kits to Metropolitan Corporation Quetta for its janitorial staff.
Installation of Hand Washing Units at Public locations
For fighting against the pandemic, the organization also joined hands with law enforcement forces for behavior change communication and installed 404 handwashing units at different public places of the province.
Coordination meetings with the government officials and stakeholders on COVID-19
For a rapid response, BRSP participated in 166 coordination meetingsat the provincial and district levels. Similarly, the organization developed a real-time data management software (4W) for the COVID-19 activities. In addition, BRSP also provided technical support to the Health department and PDMA.
The BRSP emergency and prevention activities on COVID-19 are being accomplished with the cooperation of the government of Balochistan, Indus Health Network, Al-khidmat Foundation, Metropolitan Quetta and with the financial support of international & national donors including European Union, PATRIP Foundation, Indus Health Network, UNICEF, GIZ, NRSP, and RSPN under different projects including BRACE Program, Mainstreaming Madaris Education into the mainstreaming education, and Malaria Control Program. Scientia Pakistan is proudly sharing the accomplishments of BRSP as their media partner. We are standing side by side in their efforts and working on the translation of COVID-19 precaution data and material in the regional languages of Baluchistan.
Earthquakes and the earth’s internal dynamics have long been the focus of geologists and researchers. Although humankind has achieved thousands of technological milestones, we have never been able to find a way to predict earthquakes. Geologists from the University of Maryland observed seismograph waves from earthquakes in different parts of the world over a period of about 20 years from 1990 to 2018. The number of these waves is in the thousands. This study led to some startling revelations about the Earth’s internal structure.
Courtesy; Physics. Org
Experts noticed some unusual dynamics (echos) between the molten core of the Earth’s crust and the mantle of the inner layer of the Earth’s crust, which, upon further observation, revealed a much larger and more diverse structure. This structure consists of solid and dense rocks that geologists did not know about before. The echoes revealed more widespread, heterogenous structures—areas of unusually dense, hot rock—at the core-mantle boundary than previously known. This structure is consisting of unusually dense, hot rock—deep inside the Earth below the Pacific Ocean.
For this discovery, researchers used machine learning algorithms to collect data by observing seismic waves over the next 20 years. Researchers hope that not only this discovery but also such computer-based systems will be beneficial in research on earthquakes.
“By looking at thousands of core-mantle boundary echoes at once, instead of focusing on a few at a time, as is usually done, we have gotten a totally new perspective,” said Doyeon Kim, a postdoctoral fellow in the UMD Department of Geology and the lead author of the paper. “This is showing us that the earth’s core and the mantle boundary region has lots of structures that can produce these echoes, and that was something we didn’t realize before because we only had a narrow view.”
A partial solar eclipse was observed in South Asia and Africa on 21st June 2020. In some areas, the ring of fire was also seen that left everyone mesmerized. The eclipse occurs when the Moon is too far away from the Earth to completely cover the Sun. It results in the appearance of a brightly lit ring around the darkened Moon.
Many enthusiasts captured mind-blowing photos of the phenomenon. Here are some images of the solar eclipse for your eyes to feast on!
One ring to rule them all! Eclipse from north of Bela, Baluchistan. Credit: Mehdi Hasaan
A very thin ring of fire. Credit: Zain Ahmed
Solar Eclipse as seen from Madyan Swat Khyber Pukhtoonkhowa. Credit: Imran_ullah_Miraj
A breathtaking image of the Solar eclipse shot at Karachi at 11:05am. Credit: Sayed Kawish Ali
“Ring of fire” solar eclipse pictured in China’s Tibet, Zhengzhou City and Beijing. Credit: CGTN
The dramatic ‘ring of fire’ solar eclipse as seen from Yunlin County in Taiwan on Sunday, June 21. Credit: Sam Yeh/AFP
A breathtaking picture of the phenomenon captured in Sukkur. Credit: Shaheryar Hasan
Upcoming Astronomy Events
In 2020, there are many astronomy events expected to occur. Here are a few that you should mark on your calendars.
Planet Parade: On July 11, skywatchers and stargazers will have a special treat as there will be a planet parade. Several planets like Venus, Jupiter, etc. will be in conjunction appearing to perform a parade in the skies, hence the name. It is a not to be missed event.
Perseids Meteor Shower: This is without a doubt, one of the best showers to observe as it lights up the skies beautifully. They are known for the bright meteors and are produced by the comet Swift-Tuttle. This shower runs annually from July 17 to August 24. This year, it will peak on the night of August 12 and the morning of August 13.
Mars Opposition: On October 13, Mars will be at the closest opposition to Earth and will be well lit. Astronomy lovers will have the opportunity to take beautiful snaps of the red planet. Telescopes can also be used to see the details on its surface.
Geminid Meteor Shower: Geminids is the best of meteor showers and is able to produce approximately 120 multicolored meteors per hour when it is at its peak. he shower runs annually from December 7-17. It peaks this year on the night of the 13th and morning of the 14th.
Jupiter and Saturn Conjunction: On December 21, a rare conjunction of Jupiter and Saturn will take place. It very unusual to see these two celestial giants together.