Astrophysicist Nergis Mavalvala has been named the newDean of MIT’s School of Science, effective Sept. 1. She will succeed Michael Sipser, who will return to the faculty as the Donner Professor of Mathematics, after six years of service.
Mavalvala, the Curtis and Kathleen Marble Professor of Astrophysics, is renowned for her pioneering work in gravitational-wave detection, which she conducted as a leading member of LIGO, the Laser Interferometer Gravitational-Wave Observatory. She has received numerous awards and honors for her research and teaching, and since 2015 has been the associate head of the Department of Physics. Mavalvala will be the first woman to serve as dean in the School of Science.
Quantum Astrophysicist Nargis Mavalvala in an MIT lab (Photo by Darren McCollester/for MacArthur Foundation)
Dr. Nergis Mavalvala attended the Convent of Jesus and Mary, Karachi, for her O-Level and A-Level. She moved to the United States in 1986 and enrolled at Wellesley College and got a bachelor’s degree in physics and astronomy in 1990. As a graduate student at MIT, she conducted her doctoral work under Dr. Rainer Weiss and developed a prototype laser interferometer for detecting gravitational waves. Before graduation, Nargis with her physics professor, Robert Berg, co-authored a paper in Physical Review B: Condensed Matter.
After graduate school, Dr. Mavalvala served a postdoctoral researcher and a research scientist at the California Institute of Technology, kickstarted her work with cosmic microwave background, and then eventually indulge the LIGO project. Mavalvala mainly focuses on two fields of physics: Gravitational Waves Astrophysics and quantum measurement science. She went on to do her Ph.D. in physics from MIT in 1997.
Dr. Mavalvala joined the MIT physics faculty in 2002 and was elected to the National Academy of Sciences in 2017. Born to a Parsi family, she was the younger of the two children. Her parents highly valued their daughters’ educational experiences and encouraged her to pursue higher education overseas. She was always interested in math and science and believed that she was intrinsically good at it.
Mavalval frequently questioned for gender discrimination and how she was able to break down this barrier. In an interview with the Pakistani newspaper Dawn, she states, “I grew up in a family where the stereotypical gender roles were not really observed. Everyone is capable, and I set benchmarks for all these women willing to pursue a career in STEM. Mawalwala is often viewed as a role model for aspiring female scientists of South Asian descent. In her childhood, she involved in handy work and was not bound to stereotypical gender roles in South Asian culture.
In a television interview in 2016, She stated that “When everyone has access to education, that’s when all the other things come into place. You’ve got to do what gives you pleasure, got to find a way to do it. People should just do what they enjoy most, and I think for all of society whether it’s in Pakistan or elsewhere we have to create opportunities for young girls to do what they’re good at and do what they love to do must cultivate the sense of wonder in a child.”
Mavalvala was among the team of scientists who, for the first time, observed ripples in the fabric of spacetime called gravitational waves. On February 11, 2016, the detection of gravitational waves confirmed a major prediction of Albert Einstein’s 1915 general theory of relativity. After the announcement of the observation, she became an instant celebrity scientist in her birthplace of Pakistan. Talking to the press, she claimed that “we are really witnessing the opening of a new tool for doing astronomy.”
During an interview with Pakistani newspaper Dawn, after the detection of gravitational waves, she claimed that she was baffled by the public interest in her research in Pakistan. She said, “I really thought of what I want people to know in Pakistan as I have garnered some attention there. Anybody should be able to succeed — whether you’re a woman, a religious minority, or whether you’re gay. It just doesn’t matter.”
Dr. Mavalvala has also worked on the development of exotic quantum states of light, and in particular, the generation of light in squeezed coherent states. By injecting such states into the kilometer-scale Michelson interferometer of the LIGO detectors, her group significantly improved the sensitivity of the detector by reducing quantum noise such squeezed states also have many other applications in experimental physics.
She also worked on laser cooling, where the Optical cooling of mirrors to nearly absolute zero can help eliminate measurement noise arising from thermal vibrations. Part of her work focused on the extension of laser-cooling techniques to optically cool and trap more and more massive objects, both for the LIGO project and for other applications, such as to enable observation of quantum phenomena in macroscopic objects. Prominent results from her group in this area included cooling of a centimeter-scale object to a temperature of 0.8 kelvins and inspection of a 2.7-kilogram pendulum near its quantum ground state. These experiments lay the foundations for observing quantum behavior in human-scale objects.
On February 20, 2016, Ambassador of Pakistan to the United States, Jalil Abbas Jilani, conveyed the Government of Pakistan’s message of felicitation to Nergis Mavalvala for her outstanding achievement in the field of astrophysics. She won the first Lahore Technology Award launched by Information Technology University on December 17, 2017. In 2017, the Carnegie Corporation of New York honored Mavalvala as one of its Great Immigrants awards recipients. The awards go to “naturalized citizens who have made notable contributions to the progress of American society.” In 2014, NOGLSTP recognized Nergis Mavalvala as the LGBTQ Scientist of the Year. She was awarded a MacArthur Fellowship in 2010.
Exploring the other celestial bodies for the signs of life and a new home has always been a curiosity for humankind. We have sent hundreds of probes failed and successful in learning more vividly about our solar system. Considering our search, Mars is the only planet after Earth in the habitable zone (Habitable Zone: an orbital zone in a solar/star system, where conditions for life are suitable as it’s not too cold or not hot). In scientific circles, since NASA’s Phoenix Mars lander 2008, confirmed the presence of “Water Ice” on mars, water ice means that the discovery has the same elements of waters, what we have on Earth. Scientists and Space Exploration Agencies are trying to uncover more and possibly the colonization of the neighboring planet shortly.
Humanity has tried different attempts in the past to get information and data about the fellow planet. NASA, ESA, ROSCOSMOS/Russia, CNSA/China, ISRO/India, JAXA/Japan, UAESA agencies are the among who have been trying persistently to reach the red planet through their dozens of missions in the past 50 years. Some of the main interests are to find any evidence for the past or any possible form of life there.
In this article, I will be sharing the different approaches, features, and objectives of the missions sent under different space programs by the CNSA, the UAESA and NASA last month of July.
UNITED ARAB EMIRATES SPACE AGENCY’s (UAESA) MISSION
The ambition is regarded as the ‘first interplanetary mission’ by the Arab World with the launch support of a private company in Japan. On July 20, 2020, UAESA with the help of Japanese H-IIA rocket, operated by ‘Mitsubishi Heavy Industries’ launched a spacecraft called “Hope” developed by Laboratory of Atmospheric and Space Physics (LASP) at the University of Colorado Boulder and with the support ofMohammed bin Rashid Space Centre (MBRSC).
Engineers of the Mohammed bin Rashid Space Centre work on the Hope spacecraft. Credits: UAE Space Agency
As per the UAESA, the orbiter will provide us with the first very complete picture of the Martian Atmosphere. More specifically, it will attempt to answer scientific questions such as why the martian atmosphere is losing Hydrogen and Oxygen from its atmosphere, a correlation of upper and lower atmospheric conditions will be made. Further, it will make attempts to understand and structurize a model for weather and seasonal change of the red planet. The gained information will also help scientists to understand more about the patterns and models of Earth’s atmosphere over the past millions of years.
The entire data of the mission will be shared with over 200 international universities and institutes for research and study purposes.
UAE’s ambition to transform itself from an oil-based economy into a knowledge-based economy will inspire the other rich middle-eastern countries to be a part of the “Elite Club of Space Nations”.
CHINA NATIONAL SPACE ADMINISTRATION’s (CNSA) MISSION
The People’s Republic of China, the world’s most populated country has sent a globally challenging spacecraft in the scientific race called “Tianwen-1”, this is a marvelous 5000-Kilogram robotic spacecraft consisting of an orbiter, lander, and rover. The mission was successfully launched from Wenchang Spacecraft Launch Site on 23 July 2020 and will reach in next year February 2021.
The Chinese orbiter will loop the red planet for an entire Martian year.
The orbiter will study the Martian atmosphere and particular ionosphere. A magnetic field detector will provide us with essential insights about the past magnetic field of the planet.
Interestingly, the orbiter will loop the red planet for an entire Martian year (687 days of Earth), it will act as a communication transmitting linkage between the rover and us, the rover has a lifetime of 90 martian days-typically 93 days on our planet earth.
Here, quoting David Flannery, an astrobiologist at the Queensland University of Technology in Brisbane, Australia, “The china will share the new data from Tianwen-1 with the scientific community as it shared few data sets of the moon before”. Further added, “Space belongs to everyone.”
NATIONAL AERONAUTICS AND SPACE ADMINISTRATION’s (NASA) MISSION
An illustration of NASA’s Ingenuity Mars Helicopter. Credits: NASA/JPL-Caltech
As the world’s leading space agency, the “Perseverance” is a part of the long-term endeavors of NASA’s Mars Exploration Program. This pioneering, state-of-art, scientific proposal will be two-part: first the rover, ‘Perseverance’, and a flying drone called “ingenuity”. The mission was launched on 30th July 2020 and expected to reach the Red Planet on 18th February 2021 at the ‘Jezero Crater’ a natural crater on the mars. The ultimate approach is to explore the planet from an “Astrobiological’’ aspect, searching and trying to identify the environment of the planet in the past to support any form of microbial life.
The rocks will be studied from a geological perspective to seek signs of habitability, as rocks are particularly known to preserve signs of life over-ages. Further, it’s core data collection would be “Testing oxygen production from the atmosphere” for future human landings. Besides that summing up the payload consists of around seven main instruments:
Mastcam-Z: Zoomable Paranormal Cameras
Laser Micro-Imager
A Subsurface-Radar
X-ray Spectrometer
Ultra-violet Spectrometer
MOXIE: Produces Oxygen from the Atmosphere
MEDA: A Weather Station
The curiously exciting part is the solar-powered Helicopter “Ingenuity,” which is 1.8-Kilogram, the small helicopter is expected to fly no more than 3 minutes per day and not more than five times in its 30-day flight testing period at the planet. It will serve as a foundation of a technology demonstrator for future developments of aerial vehicles for mars and other planetary bodies.
As we have discussed the aspirations of different magnitudes of Space Programs, from an infant “Hope” of the UAE to a competitive spacecraft “Tianwen-1” by the CNSA and till the end, where we can see “Perseverance” a striving instrument by the leading agency NASA, all putting their money, resources and scientific understandings for an unknown but possibly-promising future for humankind.
The Perseids meteor shower is without a doubt, one of the best showers to observe as it lights up the skies beautifully. They are known for the bright meteors and astronomy enthusiasts seek to capture the stunning phenomenon, this time of the year.
This shower runs annually from July 17 to August 24. This year, it peaked on the night of August 12 and the morning of August 13. At its peak, the display can produce as many as 150 meteors an hour. It takes place when our planet moves through the debris left by Comet Swift-Turtle.
Here are some beautiful images of the Perseids meteor shower captured around the world.
The shower seen in Gran Sasso d’Italia in L’Aquila, Italy. LORENZO DI COLA/NURPHOTO VIA GETTY IMAGES
Over the ancient city of Blaundus in Usak, Turkey, the shooting stars create a beautiful scene. ALIBEY AYDIN/ANADOLU AGENCY VIA GETTY IMAGES
The meteor streaks across the sky near the city of Ohrid, Macedonia. ROBERT ATANASOVSKI/AFP VIA GETTY IMAGES
Upcoming events
If you missed the shower, don’t worry as there are plenty of astronomy events lined up in the calendar.
Mars Opposition: In 2020 besides sending missions to Mars, we will also have it a bit near to us. On October 13, Mars will be at the closest opposition to Earth and will be well lit.
Solar Eclipse: On December 14, a total solar eclipse is expected. This phenomenon occurs when the moon blocks out the Sun’s outer atmosphere.
Geminids Meteor Shower: It is the best of meteor showers and is able to produce approximately 120 multicolored meteors per hour when it is at its peak. The shower runs annually from December 7-17. It peaks this year on the night of the 13th and morning of the 14th.
We all are aware of the ongoing pandemic crisis, be that fact or baseless WhatsApp fast forwards. But we know very little of the second pandemic we are going through “Global Mental Health Crisis” that has, to be more specific, affected greatly our healthcare professionals who have been on the frontline for almost half a year now. Unfortunately, this isn’t new to them. For doctors and paramedical staff, depression, burnouts, and excessive workloads is not a unique experience. Studies from the early 1990s found that the risk of suicide was very high among American physicians, specifically female physicians. But this time, it’s very likely for them to have elevated stress levels considering the ongoing situation.
Why are HealthCare workers most dramatically affected?
Everybody is having a hard time dealing with their mental health issues. People stuck at home in abusive relationships, patients suffering from General Health Anxiety and OCD, those who’ve lost jobs, most importantly people who’ve lost their loved ones to Covid-19. Why emphasize on health care workers?
Not starting from zero
They are not starting from the zero line. Anxiety, high stress and depression has been a part of the medical professions since times unknown. Burnouts and high workloads have already been putting their mental health at stake and a global health crisis where they’ve to endure grueling shifts, increased number of casualties to witness and difficult choices to make. Hence we are definitely not talking about sudden induced stress levels, we are talking about elevated stress levels to a point that could render a person with decreased function and exposed to addictions and drug abuse as failed coping strategies.
“Workload has doubled. I’m stressed out. But the worst was witnessing three of my young patients die of Covid. The youngest is 21, with no underlying medical condition. That took a huge toll on me.”
Difficult choices to make
Most of them had to endure the torment of making difficult choices and painful decisions. Whether that be the common question for every healthcare professional out there;
“Choosing to care for my health, my family’s health or to serve the critically ill without concerning the former options.”
Or be that the choice of which patient has to be put on a ventilator and which one can they put into arms of death, considering the shortage of ventilators and other necessary medical devices.
‘I’ve been worried about my critical patients that we can’t do much about.”
He Is a medical officer in HMC, Peshawar who has tirelessly served Coronavirus patients.
Social stigma & Public Attitude
Social distancing has been the new normal for months now. But that doesn’t necessarily mean adapting humiliating behaviors towards health care staff in your neighborhoods or in general public. This young doctor from Peshawar displayed discomfort on how they’ve been looked at while they put their lives in danger for the people around them:
“People, even close relatives, look at me in disgust only because I have served patients suffering from Covid and got infected myself and later had to go through the torment of seeing my family suffer from Covid too. All because I chose to serve my people.”
On being asked about what he had to say about the public’s attitude towards this grave condition, he enlisted all the factors that were contributing to the severity of the ongoing crisis. But to my surprise he said it had its pros too. Upon being asked he stated;
“Finally the respect has doubled. They know our importance now”.
It’s sad to know that it took us an entire pandemic to stop labeling doctors as “Butchers” and start giving health care professionals there due respect.
“This is not only work but exposure to the already hollow psychology of society, which got more obvious in these times, that makes it hard to find a reason to work out there.”
The endless guilt trips
Those who are fighting on the frontlines suffer from the guilt of putting their families at risk. While those are not on the frontline are guilty about not being there for others. They are guilty of things they don’t even control, to enlist a few; the hurdles in their career growths and job opportunities. A young ambitious doctor from Islamabad, who was about to start her job in the UK and was determined to serve people, is going through high levels of stress as this pandemic proves to be a hurdle in her way and that she has to stay home in a time where hospitals are in dire need of doctors.
“Yes it has been a hurdle. I’ve been applying for jobs in the UK. But due to the pandemic the process is extremely slow. In fact they had stopped taking doctors from outside for almost 2 months. But now the recruitment process has started again. But the uncertainty is really making me go crazy.”
The added guilt of infecting family members has elevated anxiety and doctors complain their brains are constantly in a fight-or-flight mode, which drains you out. Dr Maeeda from Cantonment General Hospital, Rawalpindi had this to say;
“It’s very stressful, worrying about getting it and bringing it home. Being strict with SOPs while a layman doesn’t care about their and our health.”
Distancing from their families
Out of the sheer fear of getting their families infected doctors and nurses had to stay away from their homes, some residing in garages and some at hotels. Not seeing or meeting your loved ones can highly affect one’s mental peace. A young doctor who got infected himself and his family members as well had to say how hard it was to stay away from his little doctors
“Had to stay away from my daughters for 45 days straight. That was very hard.”
Keeping Up with the stereotypical image
As doctors, there is a certain, stereotypical image of a calm and neutral “hide-away-your-emotions” kind of a person that they must maintain. This leads to bottling up of emotions which can have disastrous effects on doctors’ mental wellbeing. Opening up about your emotions and worries would bring along the risk of being no more a trustworthy doctor for patients. As the social stigma regarding mental health prevails here too where you are labeled crazy and not well enough to deal with patients. A proof to this is that most of the doctors I interviewed chose to stay anonymous because they had to show and portray that they are strong and unaffected and that their families might worry more after reading what they are actually going through.
Moral Injury; borrowing a military term
Moral Injury refers to an injury to an individual’s moral conscience and values resulting from an act of perceived moral transgression, which results in profound emotional guilt, shame and moral disorientation. In context to the field of medicine, it might refer to the Hippocratic Oath that each doctor takes. Moral injury in such times won’t be surprising for doctors. As a business side of the health care system and lack of proper devices e.g., a ventilator might cause doctors to make difficult choices and consequently paving a way to moral injury.
Added torment on getting your religious beliefs questioned
In Pakistan, a problem doctors faced was getting their religious belief and tawakkul questioned because they asked people to avoid congregational prayers and suggested they perform their spiritual practices at home. People refused to isolate socially and made fun of those who did by labeling them cowardly and stating they had a weak belief system. This added to the numerous factors causing distress and social humiliation to the healthcare staff.
Putting labels like weak belief systems were among the numerous factors causing distress and social humiliation to the healthcare staff.
Unhealthy behavioral patterns among healthcare professionals
Upon asking from different doctors the same question;
“How has this pandemic affected your mental health”?
“Severe insomnia. I can’t sleep at all. I’ve to take sedatives regularly. Secondly, anger issues! I was never this short-tempered. Workload has doubled. Nightmares are now regular. I try to travel to our house in Nathiagali for peace of mind even if I hardly get one day as a break.”
“My brothers, my niece, my sister in law and I myself got infected and seeing the little one suffer has taken a toll on me.”
“I’ve noticed strange behaviors and high levels of stress among my colleagues. I’ve seen some of them coming in mismatched clothes or someone brought a white shirt thinking it was his white coat. Everyone seems to go crazy. The workload is definitely taking a toll.”
“Seeing people die, especially young ones is hard. My colleagues and friends have suffered due to it but the hospitals won’t let out proper data and statistics of the doctors infected or dead.”
“Regarding mental health, it can be divided into ‘Emotional, Psychological and Social’ wellbeing. Talking in context to emotional wellbeing, doctors have emotionally collapsed. It’s not easy seeing your family, friends, and relatives die in front of you while you are unable to do anything. Now talking of psychological and social wellbeing, you can understand a person working double the shifts plus double the workload. He can’t think about spending time with your friends or family. Nobody, even your best friends, don’t want you to visit them because you’ve been assigned to a sampling unit or ICU. It is hard. No place for social or psychological well being.”
One-to-one conversations with Dr Iman Zia & Dr Hibba Noor Vardag
Dr Iman Zia is a young doctor who had the chance to work as a healthcare assistant at Field Isolation Centre at Expo, Karachi. Her sister took to social media and described her plight witnessing her sister go through tough ordeals.
She wrote in an instagram post that;
“In these awfully difficult times, where one wants to be home and safe, my sister was volunteering at the Field Isolation Centre at Expo. Risking her life to treat patients is something that takes a lot of her courage. She has been away from home for almost a month and has spent her time serving the nation.”
On asking Dr. Iman herself about how it has been for her to be on the frontline battling disease and death. She had to say this;
“Working during this pandemic has been a huge responsibility which healthcare workers have dealt with by staying calm, suppressing our emotions, for the sake of humanity. But we have been overburdened with stress, anxiety, and fear during the pandemic crisis.”
What has this pandemic changed?
“It’s surreal how this pandemic has changed people’s perception of death. How fear has replaced grief.”
What do you think about people’s attitude towards such a grave condition?
“Looking at people not following the SOPs feels miserable.”
How has it been for you and your mental health working at Field Isolation Centre Expo?
“There have been sleepless nights thinking about what happens next and feeling cranky after hours of wearing PPE. Mainly there has been a wave of fear, to avoid passing the risk of contracting the virus to our family members.”
Dr. Hibba Noor Vardag is a fresh graduate from Khyber Medical College, Peshawar. She had to start her house job at KTH, Peshawar during this pandemic. She took the start of her career in many unexpected circumstances, which definitely had its effect on her.
“How did the ongoing health crisis put your life on hold while you were about to start your job?”
“Always having a hectic schedule and then suddenly sitting at home, doing nothing had a not so good impact on my mental health. Got into unhealthy habits, over-sleeping, lesser productivity, and overthinking about every single thing which is emotionally draining.”
“You started your house job in very unexpected circumstances, how has that had an effect on you?”
“Of course it affected our career start very badly, we couldn’t practice that well, the patient influx was very low, missed all the important “busy” morning rounds and suffered from severe OCD due to the pandemic. Most importantly, our excitement got ruined.”
“How’s your learning experience suffered?”
“Currently I’m working in Gynae, the obstetrical procedures are not affected that much. But the gynecological procedures are totally at pause, so our training has been badly affected. The patients suffer a lot too.”
“How do you see your fellow doctors being affected?”
“Doctors have been exposed to a lot of sufferings during the pandemic. There is always a fear in our minds before approaching the patient who affects our output. Elective procedure on hold, training affected badly, and over our community is mentally and physically exhausted.”
Why is “Hero-worshipping” not enough? How can we help?
Social media has been flooded with posts that came out in support of our front line “heroes,” people clapping in their balconies and the government “only” appreciating our healthcare staff and numerous other ways where we’ve been hero-worshipping them. But what we need to understand is that there is a significant problem we are missing out on. Calling them heroes and clapping in appreciation is wrong on so many levels. The problem with this narrative is that it’s accentuating valor as “to work in hazardous conditions selflessly.”
While the hazardous conditions shouldn’t have existed in the first place and they exist as a result of the failed responses from government and administration bodies worldwide. This narrative creates a notion that those who are not willing to work in any more hazardous conditions to be looked down upon because they choose their safety and their family’s safety due to the scarcity of PPEs. Appreciating them and acknowledging their sacrifices is no harm, but only sticking to hero-worshipping rather than taking some concrete measures is no good.
Pay heed to what doctors and research scientists tell you. Stay home stay safe. Take care of health care professionals, reach out to them, and diminish the taboo about them being stereotypically calm while there is an entire health crisis going on.
COVID-19 has become a question of survival for not only people but industries, education systems, tourism, businesses, and even economies of countries. Healthcare systems around the world are pushed to their limits. Now and then, experimental drugs are tried by doctors to find a comfortable and better treatment for the disease. Clinical trials are run not only on pre-existing drugs but also on newly developed ones. In times like these, people look up to science for answers. Scientists and biotechnologists around the world are busy in finding potential drugs and vaccine for the disease.
As of July 6, 2020, the World Health Organization has 19 coronavirus vaccines undergoing clinical trials while the other 130 are in the pre-clinical evaluation stages. Many are still in preparation and research stages. We hope to have an effective vaccine by the end of this year or the start of the next.
Pakistan confirmed its first two cases on February 26, 2020, and it now has over 240,000 confirmed cases with a recovery rate of 56%. Pakistani scientists and academicians are also fighting against the pandemic along with academicians worldwide. Even though the country itself isn’t working on any vaccine for COVID-19, scientists of Pakistani origin are involved in some international projects. Here are a few developments in the field coming from Pakistani scientists.
NUST’s Coronavirus Testing Kit
On March 15, National University of Science and Technology, Islamabad (NUST) announced that researchers at their Atta ur Rehman School of Applied Biosciences (ASAB) had successfully established a diagnostic assay for the detection of coronavirus. The assay includes the conventional as well as real-time PCR- based methods of Syber Green and Taqman. Dr. Aneela Javed and Dr. Ali Zohaib were the researchers who worked on the kit.
This feat was achieved in collaboration with the Wuhan Institute of Virology, China, DZIF Germany, Columbia University, USA, and armed forces INstitute of pathology (AFIP), Rawalpindi.
Successful tests were performed on 330 blind samples. Finally, after testing and trials of three months, the N-CovKit has been approved by DRAP – Pakistan’s drugs and medical pieces of equipment regulating authority – for public use.
The fascinating thing about this kit is that it costs one-fourth of the imported ones and can be produced locally in any number.
Associate Professor Dr Aneela Javed and Assistant Professor Dr Ali Zohaib from NUST ASAB, worked on establishment of these assays for diagnosis of the pandemic. Courtesy: NUST
Punjab University’s Coronavirus Testing Kit
A day after NUST announced a cheap coronavirus testing kit, Punjab University announced its own that was even cheaper.
A team of scientists headed by Centre of Excellence in Molecular Biology’s Prof. Dr. Muhammad Idrees developed the diagnostic kit. Dr. Idrees, a famous virologist and ex-VC University of Hazara, said that the kits would be available in 5$ (~Rs. 800).
The estimated cost of the kit developed by NUST is around 20$ (~2000 rupees roughly).
AI-Based COVID-19 Detector
A final year student from Ghulam Ishaq Khan Institute (GIKI) claimed that he had developed an AI-based covid-19 detector that could detect positive coronavirus cases from the x-rays. This method was used by China’s Ali Baba. They could detect cases from CT scans with an accuracy of about 90%. Ali Baba did not open-source its application, so the working of the system was unknown.
Aleem independently came up with the same system with 96% accuracy for X-rays (much cheaper than CT Scans). He used a neural link and a dataset of COVID-19 positive X-rays from Dr. Joseph Pau Cohen’s GitHub repository and normal ones from Kaggle.
Drugs Research at Karachi University
International Centre for Chemical and Biological Sciences (ICCBS) at the University of Karachi has many COVID-19 projects ongoing. One made waves when Dr. Atia-ul-Wahab and her team, under the supervision of ICCBS director Dr. Iqbal Choudhry, identified nine compounds that could be used to inhibit the growth of the virus, the host cells.
Experiments of this medicine were performed at Dr. Panjwani Centre for molecular medicine and drug research, a subsidiary of ICCBS. Unfortunately, this and many more research centers were closed by the government owing to the pandemic, and hence the hunt for medicine was stalled.
In the same research center, researchers under the supervision of Dr. Zaheerul Haq and Dr. Riaz ud Din employed computational technology. They found three drugs, Remdesivir, Darunavir, and Saquinavir, to be effective against COVID19. Two other molecules were also identified. This study was published in the journal of Biomolecular structure and dynamic.
These findings were later corroborated by the US Food and Drug Administration (FDA) as it authorized doctors to use Remedesivir for the treatment of severely ill patients.
International Studies and Pakistani Scientists
Pakistan’s science and technology minister in a tweet said that 66 international studies were in progress. 43 of them focusing on vaccine development, 16 on antivirals, and re-purposed drugs while 7 on antibody-related treatments for COVID-19. He further said that Pakistan was actively contributing to these studies.
Genome Sequencing of Sars-CoV-2
Dr. Aneela Javed and Dr. Ali Zohaib from NUST’s Attaur Rehman School of Applied Biosciences (ASAB), who had also developed the diagnostic array, sequenced the entire genome of Sars-CoV-2 virus. This project was completed with the Armed Forces Institute of Pathology (AFIP), Rawalpindi, and Charite-Berin Germany. The sequence was published through the National genome Data Centre, China making it the first genome of Sars-CoV-2 to be published from Pakistan. This is now also available on NCBI, NextStrain, and GISAID.
Determining the genomic sequence was crucial for evolutionary study and accurate diagnostic assays and drug development against the virus. Efforts of NUST were also lauded by the Bureau of South and Central Asian affairs of the US state department, the US, in a tweet.
Jamil ur Rehman center for genomic research, ICCBS at Karachi University, sequenced a Sars-CoV-2 genome using the MiSeq next-generation DNA sequencing system. This sequencing identified 8 mutations as compared to the Wuhan sample. 5 such genomes have been sequenced all over Pakistan yet.
PROTECT
‘Pakistan Randomized and observational Trial for evaluation of Covid-19 treatment’ were initiated to test hydroxychloroquine efficacy alone and in combination with azithromycin and ostelmavir. Iran, Lebanon, and Sudan also opted for participating in the clinical trials.
Government College University Faisalabad’s Epitopes Research
Scientists from the Bioinformatics and Biotechnology Department of Government College University, Faislabad published research in which they used a reverse vaccinology technique for classifying surface-exposed antigens rather than focusing on the whole pathogen. T and B cell epitopes were identified through a sequence, structural and conservational analyses. Due to their prediction methods, yields, speeds, and low costs, B and T cels epitopes have become the focal point of the immunoinformatics studies. A preliminary sequence of epitopes for future vaccine developments could be seen in this study.
Dow University’s Intravenous Immuno-globulins Development
Dow University made a huge breakthrough when their research team lead by Dr. Shaukat Ali prepared hyper intra-venous immunoglobulins (H-IVIG) from the plasma obtained from recovered covid19 patients. They isolated antibodies chemically from the blood sample, purified it, and later concentrated them using ultrafiltration techniques by removing extra substances.
This was the first global report of isolation, formulation and safety demonstration of immunoglobulins purified from recovered covid19 patient. This technique is safer than conventional plasma therapy as it doesn’t risk carrying other harmful substances into the bloodstream.
Vaccine Developed By Pakistani Origin Virologist
A Pakistani origin virologist from The Lancaster University, Dr. Muhammad Munir, developed a vaccine listed by the WHO as one of the most potential ones. He also said that he had approached Pakistani authorities but couldn’t get a severe response.
Quaid-e-Azam University’s Research Identifying Vaccine Candidates
A team of researchers at the Computational Biology Lab in Centre for Bioinformatics, Quaid-e-Azam University, Islamabad headed by Dr. Syed Sikandar Azam identified novel vaccine candidates against COVID19. They utilized indigenously developed computational techniques to identify novel multi-epitopes based vaccine candidates.
The study was published in the ‘European Journal of pharmaceutical sciences. A study designing vaccination strategies that target immune responses focusing on these conserved epitopes could provide protection across beta coronaviruses.
Mobile Application To Combat COVID-19
A Pakistani technology entrepreneur, Afzal Kothari, developed an app called “COVID Track,” a real-time contact tracing app that can help steer through the health crisis. The app uses GPS services to record contact with people. When one is diagnosed with covid19, the app can tell who he has been in contact with in the past 14 days and send SMS notification. It can also determine which path or which time is safer to go out for grocery etc. The app has other additional features too.
COVID Track uses GPS services to record contact with people.
Participating in UWARN- The global Research Initiative
United World for Antiviral Research Network (UWARN) is a research initiative into infectious diseases and pandemics. Under this initiative, research organizations from six different countries, including the US, Brazil, Pakistan, Senegal, South Africa, and Taiwan will collaborate under an $8.75 million grant spread over 5 years.
Agha Khan University from Pakistan will participate in the project under the supervision of Najeeha Talat Iqbal from the Paediatrics and Child Health and Biological and Biomedical Sciences Department. Dr. Farah Qamar and Dr. Ali Faisal from the same department while Dr. Erum Khan from pathology and Laboratory Medicine are co-investigators on the project.
LUMS’ AI-Based study for COVID Drugs
Graduate students Hafsa Iftikhar and Nayyer Ali in the Biochemistry and Structural Biology Lab of LUMS led by Shahzad ul Hassan used artificial intelligence to identify potential drugs and drugs like molecules specifically targeting Sars-CoV-2 virus. The team used computational techniques to identify 3 molecules among 5000 already known drugs that could inhibit the replication of the virus.
This study has been published in ‘Computers in Medicine and Biology”. They now aim to experimentally verify the efficacy of the drugs.
UVAS-Lahore’s Sewage Water Research
Dr. Tahir Yaqub and his team at the biosafety level-3 laboratory for Emerging Pathogens of the University of Veterinary and Animal Science (UVAS), Lahore detected Sars-CoV-2 genome in sewage water and patients’ feces. This helps determine the covid19 burden in a specific area. The study was conducted in a bid to develop a smart surveillance strategy at the community level, which may add in better execution of smart lockdowns.
Medical pieces of equipment
Like many other countries, Pakistan faced a sudden shortage of medical equipment. Thanks to government efforts and devotion of local engineers, Pakistan overcame the scarcity in a short time.
Pakistan has started manufacturing oxygenators that 80% of the covid patients require. Pakistan Engineering Council has received over 53 ventilator designs, of which 13 were selected. 7 of them are in trials and will soon be mass-produced and made available for use. This will not only fulfill the local need but can also be exported to other countries.
Volunteers from all around Pakistan have come together to provide ventilators for the hospitals. ‘Open Source Venillators Pakistan’ is one such initiative under the supervision of Bahria University professor, Muhammad Umair. A prototype developed by them is currently undergoing various trials to ensure quality. The tests at Dow Medical University, Agha Khan Hospital, and Pakistan Engineering Council, Karachi, have been successful.
Other volunteers, including biomedical engineers, doctors, academics, Pakistani diasporas, resource mobilizers, and scientists called” Pakistan Against Covid19 Volunteers – PAC-V”, have also been working to develop and 3D print ventilator parts and other biomedical equipment under the supervision of Dr. Bilal Siddiqui.
The government itself has also inaugurated a ventilator production facility at NRTC. The facility has produced 15 units of indigenously developed economical and reliable portable ventilators called “SafeVent PS-100”. It can provide 250-300 ventilators monthly. This will help meet the domestic need and be exported to the rest of the world.
Recently a Lahore-based company, SPEL, has got European Union CE certification to produce face shields for healthcare professionals.
Pakistan Council for scientific and industrial Council (PCSR) has been tasked to prepare disinfectants and sanitizers. Pakistan now has sufficient sanitizers for its own people and a position to export them. PCSIR produces 1000 liters of sanitizers daily.
Local engineers also assisted in making 163+ out of service ventilators operational again. Along with these, Pakistan is already exporting masks to foreign countries.
Helping the Muslim World
Pakistan has offered its support to other Muslim countries for developing coronavirus testing kits. COMSTECH has submitted a proposal to Islamic Development Bank to enhance the testing capacity of OIC member states. The proposal aims to develop RT-Loop mediated isothermal amplification (LAMP) as well as antibodies based detection kits for covid-19 diagnosis.
While walking into a public hospital in Pakistan, one should be prepared for the depressing sights. From beds overflowing with patients to long lines of poor people seeking help for calamities that they can barely afford to fight, it seems that there is not much hope. In villages, the health facilities are scarcer and insufficient for the needs of communities. In a country where more than 70 million people live below the poverty line, health policies and the system are not coping up. No health insurance plans and rising costs of surgical procedures force many to give up and rely on divine help.
But there are many souls who think beyond themselves. They notably come forward and play their part in helping such groups and caring for their needs. Lack of healthcare is an opportunity for many welfare groups and charitable organizations to work for the vulnerable and the poor. And these support systems are heavily dependent on philanthropic contributions and make a large part of the country’s healthcare system.
The people of Pakistan are generally motivated to contribute towards philanthropic causes. In comparison to other places, there are several reasons why people are more giving. One of the most important ones includes the obligatory provision of Zakat to the deserving, a gesture much promoted and encouraged in the Muslim majority country. According to an economic survey, around 240 billion rupees were given for philanthropic efforts in 2013-14. The motivations may vary along with the accessibility and reach. Still, it is striking and incredible how much people like to give in this developing nation, which itself is marred by trials and tribulations. It is also to be noted that it is not just individuals but also other institutions from the private and corporate sectors that support the communities and non-profits with varying motives.
Health is one of the sectors where a large chunk of such contributions goes. Over the years, many new organizations have popped up that, along with the existing ones, employ an expert workforce and efficient management systems to look after the lives of those unable to afford the health facilities and treatments. They cover a variety of treatments for patients of all ages. For children, there are several renowned charitable organizations that treat malaria, birth disorders, congenital diseases, etc.
The sights in local hospitals of Pakistan are mostly depressing. Lack of services in remote areas pushes crowds to seek help at other sources. Photo by Matiullah Achakzai/News Lens Pakistan
They also cover the diagnosis and surgeries of diseases in adults like tuberculosis, diabetes, disorders of the gastrointestinal tract, heart, lungs, and kidneys. It is necessary that such services are continuously provided because the other traditional, outdated, and overburdened healthcare system cannot handle it. The quality of life in the country is very low for the vast majority of the population, and lack of healthcare services deteriorates it even more. This tends to extend and ultimately affect the workforce and the overall economy.
One of the best and perhaps the most prominent non-profit welfare organizations that contribute majorly towards the provision of health services is the Edhi Foundation. Founded by the great Pakistani philanthropist Abdul Sattar Edhi in 1951, it has become a leading provider of various facilities and is one of the largest ambulance services in the world, with more than 1800 vehicles stationed across the country. Their exemplary services are extended to providing foster homes for the abandoned and orphans and caring for those rejected by society, including those suffering from mental disorders. The mobile dispensaries of the Edhi Foundation also provide free medicines and supplies to those in need.
Talking about organizations that cater to specific individual needs, Shaukat Khanum Cancer Hospital, SIUT, and The Indus Hospital, are few of the leading providers of services that target deserving individuals with particular disorders. Cancer is one of the most widespread diseases in the country, and SKMCH is an institution that looks after the patients and provides modern therapies and consultation of experienced healthcare professionals. It runs through donations and funds generated through campaigns and with the help of committed donors. The Trust has established several centers around the country that work to diagnose and treat patients and also raise awareness through special programs. The Indus Hospital initially set up as a provider of tertiary care with 150 beds, has now grown into an extensive network. The not-for-profit entity is managed through donations and Zakat and seeks to serve the underprivileged members of the community without any discrimination. There are also centers for blood transfusion for patients with life threatening diseases like Thalassemia around the country that provide services in affordable amounts.
A call for donations for the treatment of cancer patients. Philanthropic efforts for providing healthcare services by SKMCH and other similar organizations are worth appreciating.
As mentioned before, these efforts are not just based on or work through secondary institutions. With fast online applications, many people are quick to post and call for help on social media platforms. From groups of transplant services updates to pages that feature lists and needs of those seeking help, these platforms play a significant role in propelling the movement and getting the word out. Now, with a WhatsApp status, it can take less than a minute to get collections for a deserving person, and those having influence are able to generate an even bigger impact.
There are still many people who are skeptical of the role philanthropy plays in the healthcare system. Transparency is an essential element that needs to be strengthened, and lack of it is the reason for casting clouds of doubts. Still, the confidence is somewhat there as the groups continue to use any help and assistance provided, and organizations are running well using charitable investments. The impact they generate helps in increasing visibility and encouraging others to do the same.
The allocation of GDP to the health sector is less than 1 percent. It shows that when the incentives by the government are so scant and almost non-existent, it is up to philanthropic efforts to help stabilize the troubled system and provide accessible services in rural and urban areas. The role they play is enormous and must be appreciated, but there is a long way to go. It also does not mean that the local systems should be ignored. Standards of health need to be raised sufficiently in order to compensate portions of these diverse groups and communities.
The fundamental human right to healthcare is meant for every individual regardless of their backgrounds and income group. We have seen committed groups springing up over the years to support at-risk groups who are left on their own. Life-saving surgeries and alleviation of miseries are just some of the contributions they made and are making. Disparities in the healthcare system of Pakistan need to be addressed urgently. Until then, we should continue to support as much as we can and keep encouraging the positive attitudes that can, among other things, give someone a second chance to live.
Mark your calendars, because the month of august has some amazing astronomy events in store for you. Get your telescopes and cameras ready and watch out for meteor showers, the moon, and much more.
Full Sturgeon Moon
On August 3rd, the moon will be fully lit as it will be on the opposite side of the earth as the sun, as a full moon. This was named Sturgeon Moon by early native American tribes as large sturgeon fish on ceratin lakes were easily captured during this time as compared to the rest of the year.
Perseids Meteor Shower
This is without a doubt, one of the best showers to observe as it lights up the skies beautifully. They are known for the bright meteors and are produced by the comet Swift-Tuttle. This shower runs annually from July 17 to August 24. This year, it will peak on the night of August 12 and the morning of August 13. At its peak, the display can produce as many as 150 meteors an hour. It takes place when our planet moves through the debris left by Comet Swift-Turtle
Venus at Great Western Elongation
On August 13, make sure to look low in the eastern sky a little before sunrise to witness Venus at great western elongation, which will be the maximum angle between the sun and the planet. This moment will mark Venus at an elongation of 45.8 degrees from the sun. This will be the best time to see it as it will be at its highest point above the horizon in the morning sky.
New Moon
August 19 is the day when the new moon will arise. During this event, the moon and the sun will share the elliptical longitude which means that the lunar disk is not visible from the earth. Moonlight interference will be very low which makes it the perfect time to observe faraway galaxies and clusters.
The pandemics have affected the human race throughout history with emerging and re-emerging diseases like SARS, cholera, Pandemic H1N1, MERS, yellow fever, Ebola, Zika, and drug-resistant infections. They have caused significant illness and deaths among populations in low- and middle-income countries.
About one-third of the world population was infected in 1918 by influenza and Spanish flu, and approx 50 million people died. It was estimated later that if an influenza pandemic similar in severity to the 1918 pandemic were to hit today, there could be 62 million deaths, of which 96% would be in low- and middle-income countries. Irrespective of where an outbreak starts, low-and middle-income countries always tend to bear the brunt due to fragile health systems and inadequate capacity to handle surges in cases like the current COVID-19 situation in Pakistan and many other third world countries. (According to a study published in 2019, Pakistan occupies 84th position in the third world.)
The social and economic impactof viral disease outbreaks in low and under developing countries is often more significant than would be estimated from the number of cases of disease and deaths. The impact of an epidemic depends on the direct health magnitudes and the indirect effect of disease control measures. These include social distancing interventions, such as educational sector closures, quarantine, and travel and trade restrictions. Fear-based behavior due to lack of information or reduced confidence in governments and institutions also play a role. In low and middle-income countries, grave economic disruption carries particular risks for poor households, as they may have less access to health care and lower savings to protect against financial adversity.
Epidemic outbreaks can adversely impact the economy’s long-term growth by the destruction of human capital. Human capital, mainly the manpower of a country, is considered an essential determinant of long-term growth. Furthermore, the decline in health capital, as measured in general by life expectancy, negatively affects economic growth. For example, Liberia lost 8% and Sierra Leone 7% of their healthcare workers to Ebola, with longer-term indirect effects on already weaker health systems far beyond the duration of the epidemic.
The loss of gross domestic product (GDP) is yet another undeniable reality. This was due to already poor investment and lack of prioritization of Health and Research in these countries’ budget and a significant loss in private sector growth and agricultural production, leading to concerns about food security and cross-border trade, fall in tourist numbers, etc. as restrictions on movement, goods, and services increased. The current COVID-19 Pandemic enables us to accept it with a rational approach.
A Clinic prepared for patients during the Cholera Outbreak in 2017, Bangladesh
The social and economic consequences can continue for years after an outbreak has been controlled.
Thus, ensuring effective epidemic outbreak preparedness at regional, national, and global levels is essential to protect human populations against epidemic threats and its long-lasting impacts on the country’s prosperity.
A pandemic or disease outbreak can overwhelm the health system, limiting the capacity to deliver even routine healthcare, particularly in low-resource settings. Vulnerable populations, especially the underprivileged, are more likely to suffer.
In addition to the direct impact, further social consequences can devastate weaker health systems and affected communities, undoing decades of social development. This can only be minimized when a high level of trust exists between the community and their health facilities. One aspect that is common to all control efforts, in this case, is clear, evidence-based, and specific communication with the public to rapidly and effectively trigger the response.
A lesson well-learned from history is that epidemics occur more frequently and with greater severity in crisis settings than in comparable stable situations.
When we talk about crises, we refer specifically to instances of substantially low Health Literacy, which is one of the major limiting factors in epidemic control, cause misinformation and tons of myths and lesser adherence of public to the control strategies.
Other crises may include armed conflicts like terrorism, food insecurity, mass displacement, natural disasters like floods, and/or collapse of state functions.
Another significant aspect of epidemics is they detected and reported late in these countries. Lack of public adherence to accept disease as real is yet another factor worsening it, leaving many cases unreported.
This map shows all recent outbreaks before the COVID-19, strengthening the fact that they occur all over the world
Although the history and the present situation shows that no country is safe from the threat of an outbreak irrespective of its economic, social, or geographical position in the world.
But the risk is not equal. Countries with no sound health systems and those that are fragile or conflict-affected states are at risk of the effects of outbreaks because of a lack of ability to prevent or respond to them.
To conclude, there is a dire need to keep the world safe from epidemics, serve the vulnerable, and promote health. These include sound surveillance systems so that we can detect clusters of disease and then respond rapidly to prevent spread, effective front-line reporting in communities, mutual trust, investment between the health authorities and the community, well-trained health care workers, the necessary supplies like Personal Protective Equipment (PPE), adequate investment in research and in documenting and learning from previous outbreaks.
All this development requires national commitment at both individual and government levels and often requires external international support and a strong partnership with international bodies like World Health Organization (WHO) and the Centers for Disease Control (CDC). Only this way we can lessen the impacts of outbreaks in low- and middle-income countries.
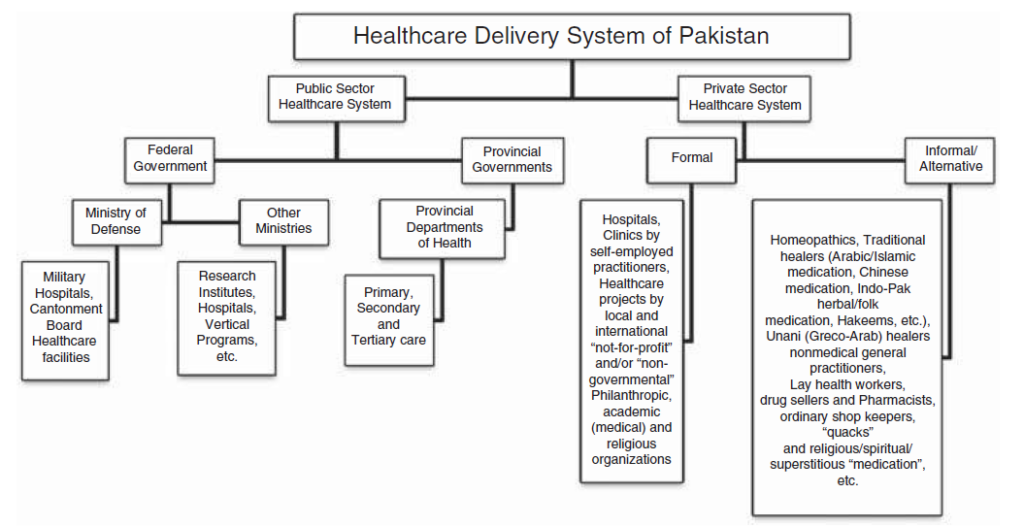
In Pakistan, the healthcare system consists of public and private sectors provided via different national programs and community health workers, and the provincial governments are mainly responsible for it. Government and semi Government organizations like the Pak armed forces, Sui Gas, Railways, WAPDA, the Employees Social Security Institution and Fauji Foundation, provide health services to their employees and their dependents through their own system.
The Government of Pakistan is spending approx 2.5 % of the GDP on healthcare, which is lower than some other Asian countries such as Sri Lanka and Bangladesh. The Healthcare portion in the Federal Budget 2020-21 is only a mere increase of 5.7% to Rs 67,484 crore from the revised estimate of Rs 63,830 crore in the previous year and falls short of the aim of spending 2.5% of GDP on healthcare. Pakistan spends 80% of its health budget on tertiary health services, which are utilized by only 15% of the population.
What healthcare statistics reveal?
The World Health Organization (WHO) ranked Pakistan 122nd in overall health system performance among 191 countries while India ranked 112, and that of Bangladesh 88 and Sri Lanka ranked 76 respectively. The health indicators, health funding, and sanitation infrastructure are commonly poor in Pakistan, mostly in rural areas. The leading causes of sickness and death include respiratory infections, congenital abnormalities, gastroenteritis, tuberculosis, malaria, diabetes, and typhoid fever.
About 19 percent of the inhabitants of adults and 30 percent of children are malnourished. The United Nations expected that in 2003, Pakistan’s HIV prevalence rate was 0.1 percent among 15 – 49, with an estimated 4,900 deaths from AIDS. Hepatitis B and C are also widespread, with approximately 3 million cases of each in the country.
Health indicators health professionals in Pakistan are identified as one of the country’s most damaged sectors, according to Transparency International surveys, the majority of Pakistani are sad with the health services they are offered. Pakistan has no national health insurance structure, and 78% of the inhabitants pay healthcare costs themselves.
Barriers and Challenges in Health care system of Pakistan
Healthcare delivery system in Pakistan
Un-satisfied Health Services/facilities in Local Community
In Pakistan’s far-flung areas, health services are not sufficiently provided due to none existence of proper healthcare infrastructure. Hospitals are not well equipped to advanced level, and healthcare centers are not fully functional under the various influence and a severe lack of funding from the Government. Public healthcare institutions that deal with critical health issues are often only placed in big cities and towns. Due to the absence of these institutions and the cost related to transportation, impoverished people living in rural and remote areas tend to consult private doctors.
Unawareness of Self-Management Approaches
Self-management hold is the help given to the community with chronic conditions that enables them to manage their health on a day-to-day basis. Self-management support can help and inspire people to learn more about their conditions and to take an active role in their health care.
Avoidably high Child and maternal Mortality
The assessment’s authors describe Pakistan’s growth as meeting the Millennium progress Goals for a falling child, and maternal Mortality indicated as “unsatisfactory.” With its population, Pakistan has extra child, fetal and maternal deaths than all but two of the world’s nations.
The report calls child survival “the most devastating and large-scale public health and humanitarian crisis Pakistan faces.” Simple actions like training more nurses and midwives (currently outnumbered by doctors could save more than 200,000 women and children in 2015.
Nutrition
Almost 40 percent of children below the age of five are underweight, and more than half are affecting by stunting. A lack of adequate nutrition for children contributes to the higher number of child and maternal deaths. Proper nutrition weakens the body’s natural defense system and ability. Only 38 % of kids are entirely breastfed for the first 6 months of life. As a result, more than half the children below five years of age lack vitamin A, 40 % are deficient in vitamin D and zinc; and nearly 62% are anemic.
Children 8 out of 10 in Pakistan do not eat the exact type and extent of food. Pakistan remains at a crisis level of acute malnutrition and is prone to natural disasters such as earthquakes & floods.
Lifestyle diseases in Pakistan
In Pakistan, as compared to South Asia, non-communicable diseases such as cancer, heart problems, and diabetes have replaced communicable diseases like diarrhea and malaria in the past 2 decades as the foremost causes of death & morbidity.
This common trend has not been coordinated by an adaptation in the Pakistani healthcare system or government policy. Poor road safety, low-priced cigarettes, and high-levels of obesity (1/4 adult) all lead to preventable deaths. The right governmental action, including higher excise taxes on cigarettes, information campaigns, walks, and new legislation could cut the premature mortality rate from cardiovascular diseases, respiratory diseases, and cancers, by 20 percent by 2025.
Low Public Spending
Crises aggravated by natural disasters like flooding, earthquakes confliction at borders, and conflict over the past decade have mobilized vast sums of money both internationally & within the country.
The corresponding sums have not been spent on vital health services, which can save many more lives. In the past, Public health spending has declined in government budgets. That has left the nation with slight support for medical costs, which are responsible for more than 2/3 major economic shock for needy families.
Lack of Innovation and Aid
Innovations are playing a significant role in the digitization of healthcare sectors worldwide. Modern technology provides an opportunity for patients and healthcare professionals to connect with each other in production environments to discuss health-related issues; on the other hand, there are fewer government funds for these kinds of projects.
Lack of Telemedicine Projects
Telemedicine is a modern technique, on the fast internet, it develops with lightning speed. After the pandemic hit the world hard, the telemedicine field is changing faster than ever before. This advanced approach helps doctors, Pharmacists, and other specialists to interact in real-time with patients in remote areas. Using a satellite, internet link, doctor or Pharmacist can sit in front of a computer laptop or mobile in any part of the country and interact with a patient.
Targeting isolated communities’ identification at a small level
Targeting communities’ identificationis a growing public health concern these days worldwide. Targeting isolated communities (TIC) at a small level is not identified in some parts of the healthcare system. Relevant electronic databases were made for these TIC and were systematically searched using an extensive search strategy to find gaps and pertinent faults to the health sector. The identification of TIC is an essential tool these days in the healthcare system to find the risk factor in the health service system.
Poverty and Health
In Pakistan, poverty is a primary reason for ill health and a barrier to access health facilities. Middle and lower-middle-class cannot purchase expensive drugs and hefty fees of specialists in big cities. The relationship is also linked to other factors, such as lack of information on suitable health-promoting practices. It is observed that tuberculosis is the most commonly emerging disease in poor nations, including Pakistan, and its treatment cost is very high.
Poor socioeconomic conditions, low health awareness, inadequate vaccination coverage, and political influence at the local community are also significant barriers in Pakistan’s health sector.
Telemedicine is a more reliable way to provide healthcare facilities to the people of the underprivileged unprocurable areas. It facilitates the patients and a doctor to communicate with a specialist 100 miles away. The history of telemedicine is ancient. In 1950, Robert Ledley used digital computers for dental projects at the National Bureau of Standards. It demands the presence of both parties at the same time and a high bandwidth communication link between them.
Video- conferencing equipment is one of the most common forms of technologies used in real-time telemedicine. The objective of telemedicine is to provide equal access to medical expertise irrespective of the geographical location of the person in need. Telemedicine has more considerable significance in developing countries since it allows people from remote areas to access medical facilities and live a healthy life.
Pakistan is one of the densely populated developing countries where most people are living in villages. There is a huge disparity in health care distribution in rural and urban areas. Pakistan spends only 2.8% of its Gross Domestic Product (GDP) on the heath.
Recent medical statistics show that the situation in Pakistan is disastrous due to a small and inadequate amount of skilled healthcare staff. According to the World Health Organization (WHO), Pakistan has one physician for 1351 people, a dentist for 20000, a nurse for 3225, a midwife for 6666, and one pharmacist for 20000. Policy emphasis continues to focus on the expansion of medical colleges, and the number grew exponentially with 2 in 1947 to 114 in 2019. [1] [2]
The fundamental structure of healthcare in Pakistan consists of rural health centers, basic health units, tehsil headquarters hospitals, district headquarters hospitals, and teaching hospitals. Here, approximately 75% of Pakistan’s population lives in rural areas, while the percentage of doctors working in those areas is about 22%. The ratio of hospital beds in rural areas to urban areas is 18% to 82%. [3]
There are also notable urban-rural discrepancies in human resources, particularly for doctors. An estimated 14.5 physicians per 10 000 population in urban areas is contrasted with 3.6 per 10 000 people in rural areas. There is a smaller but nevertheless significant discrepancy in the distribution of nurses and midwives, with a higher urban concentration of 7.6 midwives compared to 2.9 per 10 000 population in rural areas. Apart from these discrepancies, rural areas do possess a sizeable number of front-line village-based ‘Lady Health Workers’ (LHW), who act as the first point of contact for primary health care. [4]
The above statistics show that even though Pakistan’s population is mostly concentrated in the villages and small towns, the medical services in those areas are insufficient. Consult a specialist doctor, people of rural areas have no choice other than traveling to big cities. Most often than not, due to inadequate conditions of roads and traffic, the patients couldn’t meet the concerned doctor on the day of the appointment.
To provide fitting healthcare facilities to the overly frustrated rural population, the Government has to choose one of the two possible options.
To improve the poor infrastructure and attempt to build hospitals.
Telemedicine, the best option for providing the most reliable healthcare facilities using the maximum utilization of limited resources.
Telemedicine has more considerable significance in developing countries since it allows people from remote areas to access medical facilities and live a healthy life.
Telemedicine activities emerged in Pakistan in 1998 with Elixir Technology taking the initiative as a philanthropic project named TelMEDPAK, which completed small projects on an experimental basis in Taxila and Gilgit, and it got successful.
In the first project at Taxila, Ali Family Hospital, a private hospital, was equipped with a computer system and scanner with internet facilities and connected with Holy Family Hospital in Rawalpindi. Opinions were collected from the specialist doctors by sending care reports of the patients to them. The patient’s stories and records were kept strictly confidential.
The other project at Gilgit has a ‘voice chat’ facility. In this project, the telemedicine model has been demonstrated by linking District Headquarter Hospital (D.H.Q.) Gilgit, with a surgical unit of Holy Family Hospital Rawalpindi, medical specialists related to particular fields, was made available. In this regard, all the possible modalities of telemedicine were tested and practiced like sending images, x-rays, and patient records, etc. to specialists at Holy Family Hospital Rawalpindi.
Besides the private sector, the Government of Pakistan has also taken initiatives for the advancements in telemedicine. A few of them are the foundation of the telemedicine forum in September 2001, the development of health management information system (HIMS), the construction of health resource center (HIRC) which lead to the establishment of electronic patient record system at the federal hospital and promoting health research and link research respectively.
The telecommunication industry in Pakistan is undergoing rapid development as a result of which the communication connectivity all over the country has improved remarkably, and it’s a good sign for the development of telemedicine in Pakistan.
In Pakistan, numerous telemedicine setups are working in different parts of the country, being run by both Government and private organizations. In 2007, a Telehealth project was announced by Electronic Government Directorate (E.G.D.) Pakistan started in 3 Hospitals, like Mayo Hospital, Holy Family Hospital Rawalpindi, and Jinnah Post Graduate Medical Center. In 2009, Agha Khan Health Services Pakistan also started telemedicine services initially implemented in Gilgit Baltistan.
Apart from these, there are multiple Private organizations running telemedicine services in different parts of the country. The most notable of them are mentioned below;
Shifa4U
Shifa4U is a comprehensive, one-stop-shop healthcare platform for telemedicine services. In addition to online consultations with doctors, the platform allows you to schedule physical appointments for radiology, lab, homecare, and local doctors.
Aman TeleHealth
An initiative of the Aman Foundations, Aman TeleHealth, is 24-hour healthcare. The helpline provides secure and timely access to diagnostic services, basic medical advice, mental health, and family planning counseling.
Ring a Doctor
Ring a Doctor is another reliable 24/7 online consultation platform, giving you a chance to get your condition diagnosed from the comforts of your home through a video session.
Marham
Marham is a similar platform that has already served over 300,000 patients through online consultations. Offering a wide range of specialized services, Marham has a hassle-free process of connecting patients with relevant doctors and physicians online.
Sehat Kahani
Sehat Kahani boasts 3-click, 24/7 telemedicine services for those in need. It is an all-female health provider network that provides quality healthcare to those in need, using telemedicine. Sehat Kahani has a dedicated app for e-health services.
Dawaai
Dawaai.pk is an online pharmacy, allowing you to purchase all your medicines in one place. They deliver the drugs at your doorsteps without you having to go out.
Sehat
Sehat is another renowned online pharmacy, offering home delivery of prescription drugs, over the counter and readily available medicines, and special orders.
doctHERs
doctHERs provide you with 24/7 access to leading specialists and consultants through the simple convenience of a smart-phone.
Health Online
A complete healthcare web portal, catering to all your healthcare needs, Health Online (H.O.L.) offers lab tests from home, ambulance service, and an online pharmacy for the patients.
Find My Doctor
Find My Doctor is an app that connects doctors with patients. These days, two of the most essential services offered by Find My Doctor include doctor at home and lab test at home.
PIMS Online Doctor
The Pakistan Institute of Medical Sciences (PIMS) now offers its online consultation service through its official website. You can write your queries and symptoms to relevant departments, and PIMS Online Doctor will respond with the prescription, if necessary.
In Pakistan, as already discussed, Healthcare facilities are scarce compared to its population, which is approximately 220 Million, especially in rural areas. So the best way to combat this situation is to have an advanced Telehealth system that should be free of cost and readily available to masses, especially to those from the lower class and far plunged areas.
There should be a telemedicine center in each tehsil headquarter hospital, district headquarters hospital, and teaching hospital, which will provide real-time telemedicine facilities. Each of the telemedicine centers should be connected with medical stores to get the medicine in time. These telemedicine centers should then be combined with their respective provincial telemedicine centers and a centralized Telemedicine center located in Federal capital, Islamabad.
When this system gets implemented, there will be comparatively less burden on the healthcare system in hospitals. It will improve access to health care services by reducing the need for patients or doctors to travel. The people from inaccessible areas will get free of cost services when needed, and there will be comparatively mere loss of life lives, especially in case of emergencies. It will also have distinct advantages in travel emergencies in the ships, airplanes, and possibly on the battlefield.
Pakistan, being a developing country, is making advancements in telemedicine, but there is a long road ahead. The Government and private organizations should invest in the telemedicine sector to provide health care services to the people living in remote areas. Hopefully, we will be able to catch up to some of the emerging markets in integrating technology and healthcare to provide a solution to our many problems anytime soon. The healthcare providers in Pakistan are among the best in the world, if their services are utilized in telemedicine, it will be a blessing in disguise to Pakistan’s vulnerable healthcare system.